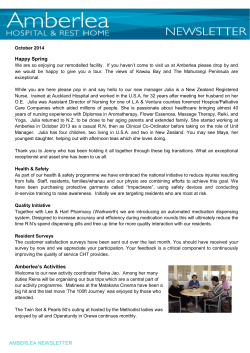
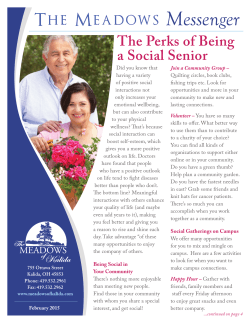
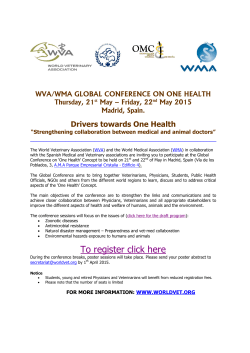
BreasWeeding During Residency: A Review of the Problems and the Solu?ons Jeanelle N. Sabourin, MD and Cathy Flood, MD Department of Obstetrics and Gynecology, University of Alberta, Edmonton, AB INTRODUCTION BREASTFEEDING RATES BARIERS TO BREASTFEEDING Subop.mal breasDeeding is a leading cause of premature mortality, disability and loss of health, according to the WHO. The Healthy People 2020 ini.a.ve has priori.zed increasing breasDeeding rates as a science-‐based objec.ve for improving the health of Americans. Residents and physicians consistently have high rates of breasDeeding ini.a.on that eventually plummet (Figure 1). The literature suggests that residents are unable to reach their personal breasDeeding goals due to workplace and occupa.onal factors (Figure 2). Cited factors include: Female medical residents and physicians have been newly iden.fied as a high-‐risk group for subop.mal breasDeeding. They oRen deny themselves and their infants of the health benefits of breasDeeding (Table 1). An increase in the number of physicians who breasDeed their own children could translate into an increase in the number of mothers in the general popula)on who breasDeed. In addi.on, female physicians that don’t reach their personal breasDeeding goals experience nega.ve emo.ons such as inadequacy, disappointment, frustra.on and depression. They also report less sa.sfac.on with breasDeeding and lower self-‐ rankings of work performance. OBJECTIVE To describe the subop.mal breasDeeding rates of medical residents, the magnitude of this problem, their barriers to breasDeeding and useful interven.ons in this specific popula.on. METHODS • Literature search using PubMed, Scopus and Web of Science up to July, 2012. • Ar.cles rela.ng to physicians and/or medical residents and breasDeeding were reviewed and summarized. RESEARCH POSTER PRESENTATION DESIGN © 2012 www.PosterPresentations.com Arthur • Inflexible work schedules with insufficient .me or breaks to breasDeed; lack of privacy or no appropriate loca.on to express milk; no refrigerator to store expressed milk; need to return to work early aRer delivery; nature of residency training (prolonged periods of .me away from their infants). Kacmar (female residents) Figure 1: Comparison of breasWeeding rates in the general popula?on (NIS 2009) and physician mothers Healthy People 2020 Goal 100 Na?onal U.S. Avg (NIS 2009) 90 Miller 81.9 80 Hutchinson 70 Riggins 60.6 60 Consequently, they may be depriving their pa)ents of these benefits as well: • Physicians with personal breasDeeding experience are more confident, comfortable and knowledgeable regarding breasDeeding promo.on. They increasingly promote this interven.on and their counseling is more effec.ve. 83 to 97% ini.a.on rate 7 to 41% at 12 months • • Sabari Merchant 50 Residency training sites oRen lack the policies and setup to facilitate breasDeeding for their trainees. BreasDeeding educa.on, although effec.ve, is not a priority in most programs. 40 34.1 30 20 Figure 2: Factors that may affect breasWeeding dura?on of physician mothers 10 0 Ini.a.on 6 months 6 months: similar for all children (58% female, 50% male) 12 months: 8% female vs. 50% male Rates according to breasDeeding inten.on (Sa4ari): • A discrepancy exists even in a mo.vated, self-‐selected group: 64% of physicians planned at least 12 months of breasDeeding but only 41% achieved this Table 1: Excess health risks associated with not breasWeeding Outcome Among full-‐term infants O..s Media Atopic Derma..s Gastrointes.nal infec.on Hospitaliza.on for lower respiratory tract disease in the first year Asthma, with family history Asthma, no family history Childhood obesity Type 2 diabetes mellitus Acute lymphocy.c leukemia Acute myelogenous leukemia Sudden infant death syndrome Among preterm infants Necro.zing enterocoli.s Among mothers Breast cancer Ovarian cancer From: Breas?eeding Medicine. 2010;5(1):35-‐39 Excess Risk (%) 100 47 178 257 67 35 32 64 23 18 56 138 4 27 Adapted from: U.S. Department of Health and Human Services. The surgeon general's call to ac)on to support breas?eeding. 2011. • Educate your residents, faculty and allied staff about the benefits and importance of breasDeeding (for themselves and their pa.ents). • Encourage breasDeeding by all your colleagues. • Have a wriben policy to support breasDeeding in your program/at your teaching site. • Provide adequate maternity leave and flexible schedules whenever possible. • Approve and encourage frequent ‘breasDeeding breaks’ for nursing residents, especially when in surgery or on-‐ call. • Ensure appropriate, designated loca.ons to express and store milk. • Provide breast pump if possible. • Rooms should be close-‐by and convenient. • A phone and a network computer allows residents to answer pages and facilitates con.nuity of care. CONCLUSIONS 12 months Rates according to resident gender (Kacmar): • • RECOMMENDATIONS TO SUPPORT BREASTFEEDING AMONG RESIDENTS INTERVENTIONS No interven.ons other than educa.on have been studied in physicians and residents. Studies show that: • Increasing the amount of breasDeeding educa.on and training in pediatric residency curriculums improves knowledge, confidence and prac.ce paberns related to breasDeeding. • A higher exclusive breasDeeding rate was noted in all infants born at ins.tu.ons where an educa.onal program for trainees was integrated. The interven.ons should address the specific barriers iden.fied for this high-‐risk group. A flexible schedule and longer maternity leave may promote ongoing breasDeeding for residents. Although breasDeeding ini.a.on is very common for female residents, the con.nua.on rate steadily decreases with .me. This appears to be due to work-‐related factors. Although workplace interven.ons have been suggested and improving breasDeeding rates in female residents will provide short and long-‐term health benefits for them, their infants and also their pa.ents, few have been studied. SELECTED REFERENCES • Healthy People 2020 topics & objec.ves: Maternal, infant and child health. www.healthypeople.gov/2020/topicsobjec.ves2020/ Updated 2012. • Anchondo I, Berkeley L, Mulla ZD, et al. Pediatricians', obstetricians', gynecologists', and family medicine physicians' experiences with and aotudes about breast-‐feeding. South Med J. 2012;105(5):243-‐248 • Goldstein AO, Freed GL. Breast-‐feeding counseling prac.ces of family prac.ce residents. Fam Med. 1993;25(8):524-‐529 • Hutchinson AM, Anderson NS,3rd, Gochnour GL, Stewart C. Pregnancy and childbirth during family medicine residency training. Fam Med. 2011;43(3): 160-‐165 • Kacmar JE, Taylor JS, Nothnagle M, Stumpff J. BreasDeeding prac.ces of resident physicians in Rhode Island. Med Health R I. 2006;89(7):230-‐231 • Miller NH, Miller DJ, Chism M. BreasDeeding prac.ces among resident physicians. Pediatrics. 1996;98(3 Pt 1):434-‐437 • Riggins C, Rosenman MB, Szucs KA. BreasDeeding experiences among physicians. Breas?eed Med. 2011 • Sabari M, Levine D, Serwint JR. Physician mothers: An unlikely high risk group-‐call for ac.on. Breas?eeding Medicine. 2010;5(1):35-‐39 • Sabari M, Levine D, Bertram A, Serwint JR. BreasDeeding inten.ons of female physicians. Breas?eed Med. 2010;5(6):297-‐302. • Walsh A, Gold M, Jensen P, Jedrzkiewicz M. Motherhood during residency training: Challenges and strategies. Can Fam Physician. 2005;51:990-‐991
© Copyright 2026 ExpyDoc