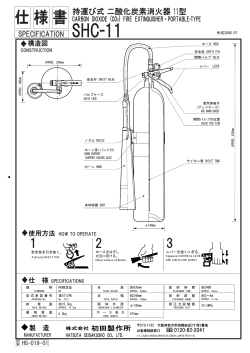
Journal of the association of physicians of india • vol 62 • published on 1st of every month 1st july, 2014 53 PICTORIAL CME’s The Quadricuspid Aortic Valve Ankush Sachdeva*, Biswajit Paul**, AK Omar*** Fig. 1 : Transesophageal echo showing zoomed color compare image of quadricuspid aortic valve (type G-star marks showing four unequal cusps) and aortic regurgitation jet arising from central area of non-coaptation. A * Attending Cardiologist, Consultant Cardiologist, *** Director Non-invasive Cardiology and H.O.D. Heart Command and Emergency, Fortis Escorts Heart Institute, Okhla, New Delhi Received: 01.11.2012; Accepted: 19.11.2012 ** © JAPI • july 2014 • VOL. 62 47 year old female was diagnosed to have moderate to severe aortic regurgitation on transthoracic echocardiogram and referred to our institute for an aortic valve replacement. She had no previous history of cardiovascular disease and had complaints of recent progressive dyspnea. There was no history of angina or syncope. Her blood pressure was 150/60 mmHg and auscultation revealed a diastolic murmur at aortic area. Her transthoracic echocardiography was repeated which confirmed the presence of significant aortic regurgitation and left ventricular dilatation with a mild left ventricular dysfunction.A transesophageal echo was done to look into the morphology of aortic valve w h i c h s h o we d q u a d r i c u s p i d a o r t i c valve(QAV) with four unequal sized cusps(type G) and a central area of non-coaptation leading to moderate to severe aortic regurgitation (Figure 1).The coronary angiogram was normal and no associated cardiac anomaly was found. Patient underwent a successful aortic valve replacement using a bileaflet mechanical valve prosthesis. Quadricuspid aortic valve is a rare entity and warrants a serious evaluation rather than academic interest. The estimated incidence is 0.008 to 1.0% of all congenital heart disease. 1 Aortic regurgitation is the commonest hemodynamic abnormality associated with QAV due to non-coaptation of the cusps and aortic stenosis is rare. Hurwitz and Roberts in 1973 classified the QAV according to their anatomical variation. 2 Seven variations were described by them; A=four equal cusps, B=three equal cusps and one smaller cusp, C=two equal larger and two equal smaller cusp, D=one large, two intermediate and one small cusp, E=three equal cusps and one larger cusp, F=two equal larger and two unequal smaller cusps and G= four unequal cusps. Most common type is type A, unlike our patient which showed a type G variant which is rare. Coronary anomalies are most frequently associated with a QAV and sometimes atrial and ventricular defects, patent ductus arteriosus and 605 54 Journal of the association of physicians of india • vol 62 • published on 1st of every month 1st july, 2014 other anomalies have been reported. QAV is most often functionally abnormal and requires surgery. 606 References 1. Feldman BJ, Khanderia BK, Warner CA, Serward JB, Taylor CL, Tajik Aj : Incidence,description and functional assessment of isolated quadricuspid aortic valve. AMJ Cardiol 1990;54:937-938 2. Hurwitz LE, Roberts WC. Quadricuspid semilunar valve. Am J Cardiol 1973;31:623-626. © JAPI • july 2014 • VOL. 62
© Copyright 2026 ExpyDoc