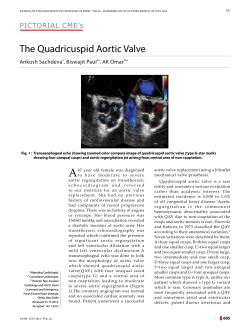
Aortic Diseases Geneviève Derumeaux, FESC Henri Mondor Hospital, APHP Créteil France European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 2014 ESC Guidelines on the Diagnosis & Treatment of AORTIC DISEASES Chairpersons: Raimund Erbel (Germany) & Victor Aboyans (France) - Acute aortic syndrome Aortic aneurysm Genetic aortic diseases Congenital diseases like aortic coarctation Atherosclerotic lesions Aortitis and aortic tumors 2014 version www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Acute Aortic Syndromes (AAS) Ï Acute aortic dissection (AAD) Ï Intramural hematoma (IMH) Ï Penetrating aortic ulcer (PAU) Ï Aortic pseudoaneurysm Ï (Contained) rupture of aortic aneurysm Ï Traumatic aortic injury 1. Diagnosis challenging 2. Untreated may be rapidly deadly www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Class 1: Classic AD Class 2: Intramural haematoma (IMH) Classification of Acute Aortic Syndromes (AAS) According to Pathophysiology Class 3: Subtle or discrete AD www.escardio.org/guidelines with bulging of the aortic wall European Heart Journal Class 4: Penetrating aortic(2014):doi:10.1093/eurheartj/ehu281 ulcer (PAU) Class 5: Iatrogenic/traumatic AD www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Clinical Presentations and Complications of AAD www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Laboratory Testing in Suspected AD D –Dimers • Should always be considered along with the pretest clinical probability • Immediately very high in AAD • May be negative in IMH and PAU www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Clinical Probability Score of AAS Risk score 0-3 according to the number of positive categories (1 point per column) www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases Breakthrough due to Imaging followed by new Treatment Options Landmarks for Imaging the Aorta www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases - Imaging Techniques - For work up usually more than one technique is used www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases - Recommendations for Imaging - www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Decision-Making in Patients with Suspected AD www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Recommendations for Diagnostic Work-Up in AAS www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Recommendations for Diagnostic Work-Up in AAS www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Treatment of Acute Type-A AD Ï Untreated 50% mortality within 48 hours, 90% at 1 month. Ï Urgent surgery treatment of choice → 25% perioperative mortality, 18% neurologic complications → age increases the perioperative morbidity and mortality but age per se not an exclusion criterion for surgery. → controversial for patients with major neurologic deficit or coma; prognosis poorer but recovery possible if time from symptom onset to surgery <5 hours. Ï Mesenteric malperfusion → surgical/hybrid approach, fenestration of the intimal flap. www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Treatment of Complicated Type-B AD Ï Ï Ï Persisting/recurrent pain, uncontrolled TEAVAR in Type-B AD HTN on full medication, early aortic expansion, malperfusion, signs of rupture (haemothorax, periaortic and mediastinal hematoma↑) Thoracic endovascular aortic repair (TEVAR) treatment of choice →closure of the primary entry tear → decompression and thrombosis of the false lumen → malperfusion (if present) may resolve → aortic remodeling and stabilization Nienaber CA et al. Circ Cardiovasc Interv. 2013;6:407-16 Surgery reserved for patients not candidate for TEVAR www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Treatment of Uncomplicated Type-B AD Ï Medical therapy to control pain and blood pressure Ï Repetitive imaging (MRI/CT) Ï TEVAR → INSTEAD (XL) trials • 140 pts, randomized TEVAR + OMT vs OMT alone • At 2 y TEVAR better aortic remodeling but no difference in mortality • Retrospective analysis of extended FU at 5y www.escardio.org/guidelines Progression plus aorta-related adverse events (deaths, conversion, ancillary interventions) European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 INSTEAD-XL Trial: TEVAR vs. Medical Management in Stable Type-B AD 11.1% versus 19.3% All-cause mortality 6.9% versus 19.3% Aorta-specific mortality Nienaber CA et al. Circ Cardiovasc Interv. 2013;6:407-416 www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Treatment of Type A/B Acute Aortic Dissection www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 TEVAR for Acute Aortic Syndromes Indications for TEVAR www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 TEVAR for Acute Aortic Syndromes Indications for TEVAR Recommendation for management of intramural haematoma(IMH) (TAI) www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases (Thoracic) Endovascular Aortic Repair (T)EVAR ((T)EVAR www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Follow-up after thoracic aortic intervention (1) Ï Clinical and imaging are both necessary to limit and detect complications, not only at the operated site but also the remaining aorta. Ï After TEVAR or surgical thoracic aortic repair, first F-U should be performed at 1 month to exclude the presence of early complications. Surveillance should be repeated. Ï Follow-up includes risk factors control. Blood pressure should be monitored closely, as >50% of cases may have resistant hypertension. www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Follow-up after thoracic aortic intervention (2) Ï If, after TEVAR for TAA, patients show a stable course without evidence of endoleak over 24 months, it may be safe to extend imaging intervals to every 2 years; however, clinical follow-up of the patient´s symptom status and accompanying medical therapy should be maintained at yearly intervals. Ï Patients with TEVAR for AD should receive yearly imaging, since the FL of the abdominal aorta is usually patent and prone to disease progression. www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Follow-up www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Intramural Hematoma (IMH) Ï Hematoma develops in the media of the aortic wall in the absence of a false lumen or intimal tear. Ï Diagnosis: circular or crescentic thickening >5 mm of the aortic wall in the absence of detectable blood flow. Ï 10-25% of AAS – 30% ascending aorta Type-A IMH – 10% arch – 60-70% descending TA (Type-B IMH) www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Intramural Hematoma (IMH) Ï Diagnosis → CT/MRI – Unenhanced acquisition + contrast-enhanced aquisition in CT → sensitivity 96% Ï Type-A IMH – In-hospital mortality similar to type-A AD – 30-40% evolve into AD Ï Type-B IMH – In-hospital mortality similar to type-B AD www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Predictors of IMH Complications www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Management of Intramural Hematoma (IMH) Complicated IMH → recurrent pain, IMH expasion, periaortic hemantoma, tears www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Penetrating Aortic Ulcer (PAU) Ï Ulceration of an atherosclerotic plaque penetrating through the internal elastic lamina into the media. Ï 2-7% of all AAS. Ï Propagation → IMH, pseudoaneurysm, aortic rupture, AD. Ï Natural history: progressive TAA. Ï Most commonly located in the middle and lower distal thoracic aorta (type-B PAU). Ï Elderly patients, smokers, HTN, associated CAD, COPD, AAA Ï Diagnosis → unenehanced/contrast enhanced CT www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Management of Penetrating Aortic Ulcer (PAU) Complicated PAU → Refractory pain or signs of contained rupture (rapidly growing ulcer, periaortic hematoma, pleural effusion) www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Conclusions Acute Thoracic Aortic Syndromes (1) Ï Potentially deadly but at the same time treatable conditions to be considered in the differential diagnosis of acute chest pain. Ï Decision making in suspected AAS should be based on the a priori probability based on a clinical score and according to the score results it should include biomarkers (D-dimers) and imaging. Ï TTE: initial imaging investigation, frequently complemented by TOE/CT/MRI. Ï Type-A AD → urgent surgery. Ï Type-B AD → complicated →TEVAR → uncomplicated →TEVAR to be considered. www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 Conclusions Acute Thoracic Aortic Syndromes (2) Ï IMH – Type-A → surgery recommended – Type-B → OMT; if complicated TEVAR should be considered Ï PAU – Type-A → surgery should be considered – Type-B → OMT; if complicated TEVAR should be considered Ï (Contained) rupture of TAA and traumatic aortic injury – If anatomy favorable and expertise available → TEVAR preferred over surgery www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281 2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases - Summary Holistic view on the aortic disease Close cooperation of many experts for diagnosis and treatment Create Aortic clinics and Aorta Teams Imaging by TTE/TOE, CT and MRI corner stones search for land marks Medical therapy follows disease aetiology Endovascular treatment breakthrough Surgery provides new technology www.escardio.org/guidelines European Heart Journal (2014):doi:10.1093/eurheartj/ehu281
© Copyright 2026 ExpyDoc