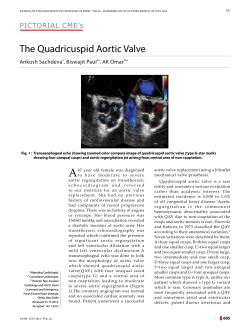
ISSUE 85 A f f i l i a t e d t o t h e B r i t i s h C a rd i o v a s c u l a r S o c i e t y i n c o r p o ra t i n g t h e B S E N E W S L E T T E R CONTENTS include: Ventricular septal rupture complicating acute myocardial infarction 5 Cardiology Training in Core ECHO: The Good the Bad and the Ugly 6-9 Front Cover 9 Uni to Quinti The Spectrum of Aortic Valves 10 - 13 New Guidelines: A Guideline Protocol for the assessment of Restrictive Cardiomyopathy 14 - 20 MARCH 2014 2013/14 BSE COUNCIL MEMBERS ECHO ISSUE 85 MARCH 2014 CONTENTS Page 4 Presidents Message Page 5 Ventricular septal rupture complicating acute myocardial infarction Page 6 - 9 Page 9 Cardiology Training in Core ECHO: The Good the Bad and the Ugly Front Cover Page 10 - 13 Uni to Quinti The Spectrum of Aortic Valves Page 14 - 20 New Guidelines: A Guideline Protocol for the assessment of Restrictive Cardiomyopathy Page 21 - 26 Case Reports Page 27 Conference Report Page 28 - 30 Echo in Africa Page 30 Letter to the Editor Page 31 Lifetime Achievement Award Page 32 BSE Practical Competence Assessment Pilot Page 33 BSE Wordsearch Page 34 - 35 Recently Accredited Members Page 35 Dates for your Diary Page 36 Call for Abstracts 2014 OFFICERS President: Dr Guy Lloyd President Elect: Dr Rick Steeds Vice President: Jane Allen Honorary Secretary: Jude Skipper Honorary Treasurer: Tracy Ryan ELECTED MEMBERS Gurpal Bhogal Dr Adelle Dawson Dr P Rachael James Jane Lynch Dr Jamil Mayet Dr Thomas Mathew Dr Jim Newton Keith Pearce Dr Bushra Rana Dr Rick Steeds Eastbourne DGH University Hospital Birmingham York Teaching Hospital Queen’s Hospital, Essex Walsall Manor DGH Russells Hall Hospital, Dudley Ninewells Hospital, Dundee Royal Sussex County Hospital Wythenshawe Hospital, Manchester St Mary’s Hospital, London Nottingham City Hospital John Radcliffe Hospital, Oxford Wythenshawe Hospital, Manchester Papworth Hospital University Hospital, Birmingham CO-OPTED MEMBERS (1 year term) Dr Chris Eggett SCST Representative, Freeman Hospital Newcastle Dr Nick Fletcher ACTA Representative, St. George’s Hospital, London Nicky Mills Industry Representative, Bracco UK Dr Mark Monaghan Kings College Hospital, London Dr Muttucumarasamy Mahendran Primary Care Representative, Milton Keynes Helen Rimington Academy of Healthcare Science Representative Dr Rizwan Sarwar Jr Dr Representative, John Radcliffe Hospital, Oxford Stefanie Bruemmer-Smith Brighton & Sussex Hospital, ICS Representative Gill Wharton Academy CVRSGUI Professional Group Representative Dr Gordon Williams ECHO Editor York Teaching Hospital INSTRUCTIONS TO AUTHORS ECHO is published four times per year. It is the official publication of the British Society of Echocardiography the contact address is: BSE Administration, Docklands Business Centre, 10-16 Tiller Road, Docklands, London E14 8PX, Tel. 020 7345 5185, Fax 020 7345 5186 Email [email protected]. Members of the society are invited to submit articles, case reports or letter correspondence. Submissions should be to ‘The Editor’, ECHO and forwarded by email to: [email protected] and copied to [email protected] . The format should be text as a normal word document and images supplied as high resolution jpeg, tiff, eps or pdf files. Other formats including powerpoint or of web image construction may result in reduced resolution and may be unacceptable. Articles should contain appropriate references. References to be constructed with the first two authors, thereafter abbreviate to ‘et al’, then article title, followed by journal reference. Submissions to ECHO are currently not peer reviewed but may soon become so, changes will be advised. The Editor has discretion on acceptance. Patient consent is required for case reports. It should be noted that opinions expressed in articles or letters are the opinions of the author(s) and not of the council of the British Society of Echocardiography (BSE). Official BSE council views or statements will be identified as such. Information in respect of advertisements can be obtained from [email protected]. Editor PA G E 3 PRESIDENT’S MESSAGE N equals one Earlier this year something momentous happened. After many years of meetings, lobbying, pressure, arguments, frustration and disappointment, the first clinical scientist was officially registered with the Academy for Healthcare Science. Brian Campbell, President of SCST is the n equals one. The importance of this cannot be overstated. After so long, there is now a process whereby clinical scientists can gain professional recognition. This opens the door for clinical scientists to play an even more pivotal role in frontline patient care, and also sets the stage for the consultant clinical scientists who will be produced by the Higher Scientific Specialty Training programs. As graduates from Modernising Scientific Careers will automatically be entered on to the register, this will over time become the clear route to professional recognition. There is of course a “but” at this point. While the path is clear for those coming through the MSC approach, it is much less clear for those already within the profession. The MSC equivalence route is currently in its trial period, this was the route by which Brian Campbell was registered, and all areas of cardiovascular physiology have been asked to provide a candidate to test the process. Jane Allen, Vice President of BSE is currently going through that system and this should provide valuable insights for those wishing to follow her. Ultimately over a five year period those who wish to make the transition should be able to. The requirements are posted on the Academy website and it is fair to say that at present the process is quite onerous. The BSE is lucky to have great representation at all levels in the Academy which means that we have been instrumental in forming some of the processes and we also get a heads up on developments well in advance. Because many members of our society do not necessarily possess the academic modules required by equivalence this will present some problems and there will be more PA G E 4 than one option for them. It is likely that Higher Education Institutions will begin to offer academic modules to allow the current workforce to top up their portfolio to reach the equivalence criteria. The RCCP voluntary register will also continue allowing an alternative route for those who are not aiming for equivalence through the academy. The one area about which the BSE remains resolved is that echocardiography should not be part of the Practitioner role. In other news After an unprecedented early response, there are still places available for the Echo in Africa program. We are really keen to get as many members of the society involved either by volunteering or by fundraising for this ambitious and worthwhile initiative. A range of events will be announced soon and the fundraising will extend into next year (this is a more than one year endeavor). The website will be up and running in the near future and just giving accounts for those who wish to fundraise will also be available in the next few weeks. Those who wish to contribute at the time of their subscription renewal will have the opportunity to do so. It is that time when council considers nominations for the Life achievement award. Potential recipients are nominated by the membership and decided by council and conferred both the award and life membership. I would therefore invite members to nominate those that have made an outstanding contribution to join Gill Wharton and Graham Leech, previous worthy awardees. To nominate someone email [email protected] by 27th June 2014. Finally, I am delighted to be able to formally announce that Rick Steeds was elected unopposed as the next President of BSE and will take over the rein after the AGM in October. Rick has been a tireless contributor to the society and been instrumental in shaping so much that we take for granted. Most recently he has presided over an unparalleled increase in the educational output of the BSE, chairing this committee. He won’t need it, but, I wish him the best of luck nonetheless. Guy Lloyd, President VENTRICULAR SEPTAL RUPTURE COMPLICATING ACUTE MYOCARDIAL INFARCTION Interventricular septal rupture is an infrequent complication of acute myocardial infarction in the thrombolysis era, complicating around 0.2% of ST elevation myocardial infarctions and is associated with a high mortality (74%) (Crenshaw et al). Patients typically present with cardiogenic shock associated with a new harsh, pan-systolic murmur one to five days following myocardial infarction. Post infarct ventricular septal defects (VSD’s) are usually associated with occlusion of the left anterior descending artery (LAD) whereby the septal defect is located in the mid to apical septum, although occasionally (as in this case), they are a result of non-LAD occlusion, typically affecting the basal infero-septum. The borders of the defect comprise friable, necrotic myocardium and the size of the defect can range from <1cm to several centimetres. The size of the defect determines the degree of left to right shunting and in turn, the likelihood of survival. Clinically, ventricular septal rupture should be considered in the post-infarct patient with a sudden deterioration several days following admission in the presence of a loud, pan-systolic murmur. In patients with cardiogenic shock, death is virtually inevitable without definitive surgical treatment. Surgical patch repair of the defect is challenging due to the friable nature of the tissue surrounding the defect. Device closure has been reported but its use is currently reserved for those considered Legend: Colour Doppler flow imaging highlighting the intraventricular septal rupture. not suitable for cardiac surgical intervention. VSD’s can be small and, especially if located apically, difficult Reference to identify on transthoracic imaging. For this reason, the sonographer must have a high index of suspicion for the presence of a VSD rupture whilst performing the scan. The use of off-axis views and colour Doppler may be helpful in Crenshaw BS, Granger CB, Birnbaum Y, Pieper KS, Morris DC, Kleiman NS, Vahanian A, Califf RM, Topol EJ Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial demonstrating the defect. infarction. GUSTO-I (Global Utilization of Streptokinase and Laura Dobson Monashheart, Melbourne, Australia TPA for Occluded Coronary Arteries) Trial Investigators. Circulation. 2000;101(1):27. PA G E 5 CARDIOLOGY TRAINING in CORE ECHO: The Good the Bad and the Ugly Introduction Last year, the GMC and BJCA (British Junior Cardiac Association) national surveys, highlighted major failings in training in echocardiography. Concerned by this, the SAC (Specialist Advisory Committee) approached the BSE to investigate and understand the reasons why this was the case. The BSE in conjunction with the BJCA held a joint training day. Over 100 Cardiology trainees attended. The day included a debate and discussion. In this report we highlight the current barriers to achieving high quality training, identify the major stakeholders and consider how UK core echocardiography training can be improved. Current Training Format It is generally agreed that of all the core skills, being able to perform a transthoracic echocardiogram is the most crucial for patient management, service delivery and education. The transthoracic echo is an easily accessible bedside investigation, which is not only cost effective but allows rapid acquisition of complex data, accelerating diagnosis and further management. At a time where the pressures on the NHS continue to intensify, timely decision-making is key. Limitations in high quality service delivery hamper patient care in multiple ways and can in part be attributed to standards in doctor training and acquisition of essential core specialty skills. With the introduction of Modernising Medical Careers, reducing total training time by one year, and implementation of the New Deal and Working Time Regulations, the working time has been restricted to an average of no more than 48 hours per week. Although these changes offer benefits, they also present a number of challenges; in particular those resulting from tensions between demands for service provision (with increasing on-call commitments) and training. The requirements for core echocardiography training are specified in the new cardiology curriculum, first introduced in 2007 and updated in 2010; it sets out a clear framework of knowledge and skills. Trainees must acquire an understanding of the role of echocardiography in managing patients with cardiac disease; be able to perform, interpret and report a transthoracic study; and understand the indications of more advanced techniques including TOE and stress echocardiography. Currently practical competency (including interpretation and reporting skills) can be demonstrated through completing six directly observed procedural skills assessments (DOPS) or by achieving BSE transthoracic echocardiography accreditation. See table 1. The Issues with current Training The key issues center around access to formal echo training lists. At present there is variability in whether a local echo PA G E 6 trainer is identified to over see the delivery of hands-on structured training. It seems a lack of a named local echo-trainer has a negative impact on the quality of training received. Trainees have also highlighted inconsistencies of Regional Training Committee expectations of what constitutes core training in echocardiography and the level of support provide to the trainee in achieving these goals. Echo departments are expected to deliver the practical aspects of core echo training. However, StR training lists are disrupted by lack of protected time, where StR’s may fail to attend a training list due to demands elsewhere. Understandably, such lists are then given out reluctantly. There is a lack of engagement of senior physiologists in the formal training programme, yet they are the very people who are expected to deliver the training. It is not surprising that this aspect of cardiology training has been highlighted as a major failing, since it is the only procedure based training where, at a local level, senior doctors rarely become involved. While the training from clinical scientists results in high quality tuition, the lack of medical input affects the attitudes and culture; resulting in deprioritization of echo training. The Way Forward After discussions with SAC, BCS Training Committee and BJCA, the BSE have suggested the next steps in how these issues might begin to be addressed. This is summarized in a letter to the Cardiology SAC and a response is currently awaited. What is clear is the three key stakeholders(the trainee, the specialist training committee (STC) led by the Training Programme Director (TPD), and the hospital/echo lab) all play an active role in training registrars.Additionally the BSE have a key role in facilitating the process.However, there appears to be inconsistencies and confusion in understanding exactly what is expected of each.It would be useful to re-iterate and clarify these roles; not only to aid the trainees and those responsible for training them, as to what they should expect from each other, but also what they must contribute. A summary of these suggestions is given in table 2. Some of these points are discussed in more detail below.A more detailed account will be published in the fourth coming BSE journal ‘Echo: Research and Practice’, due to be launched in the coming months. 1. Better access to echocardiography sessions with appropriate supervision and training. A lack of access to a regular supervised echocardiography training list(s) is perceived as one of the major barriers to achieving good quality training. The reasons for this are complex. Although some trainees reported very few, or even no specific training lists offered by echocardiography departments, in many cases an increased demand and prioritisation of service commitments and constraints of shift-patterns led to an inability to attend available sessions. Training sessions delivered were usually not ‘bleep free’ protected time.Furthermore, trainees felt that they were not prioritised due to a number of reasons; staffing constraints, the need to allocate training lists to trainee physiologists, the significant impact of training on general workflow. However what is also clear is that non-attendance of Table 1 How to demonstrate competency in core echocardiography BSE Transthoracic Accreditation • Written exam • Logbook of 250 cases (with specific case mix) collected over 24 months before and after passing exam Directly Observed Procedure (DOPS) Assessment • A minimum of 6 DOPS completed by at least 2 different assessors • BSE curriculum assessment tool (not mandatory) • Logbook (not mandatory) Table 2 Stakeholder Regional Training Committee • Should provide trainees with clear guidance of what to expect from their local echocardiography departments, including named echocardiography mentor, responsible for hands-on training and a regular ‘protected time’ (min 1x/week) training lists with supervision from a physiologist (ideally BSE accredited) or cardiologist. • Clear guidance as to how to achieve structured training and experience eg BSE accreditation process. • A regionally appointed echo training director to over see oversee training • A regionally appointed physiologist to support and facilitate training delivery across the region • Clear guidance to the trainee as to the appropriate pathway to raise concerns Local Echocardiography Department/Hospital Trust • Should offer a formal supervised training session in TTE • Should identify a training lead (physiologist and/or cardiologist) responsible for ensuring echo training delivery Trainees • Should know exactly what is expected of them during core echo training (eg producing evidence through case logbook collection. BJCA echocardiography toolkit provides a succinct summary of training requirements and proposed time line to achieve this)11 • Should highlight any issues regarding difficulty in acquiring competencies early in the training process to allow relevant actions to be taken using the pathway provided by the STC British Society of Echocardiography • Should support the delivery of high quality echocardiography training through - National BSE training days in addition to proposed regional echocardiography courses for core trainees which will include both core knowledge and simulator training - Greater emphasis on echocardiography training at BSE conference - Raising awareness (and offering support) amongst physiologists of the importance and benefits of training cardiologists - Develop an updated version of the curriculum based assessment to be submitted in conjunction with DOPS assessment to achieve core competency - Development of formal recommendations for guidance on training cardiologists in echocardiography in the UK an allocated training echo list as an option isn’t acceptable; and leaves the echo department in difficulties. Therefore any reluctance on the part of the echo department is understandable. Therefore, there requires a shift in attitudes, where the STC clearly mandates the trainee to demonstrate attendance at echo lists; it would be worth knowing this is in fact already an expectation in the training programme. The STC should then actively seek evidence from the trainee that this is occurring. The hospital staff, from the consultants to the echo department, acknowledge the mandate to provide a regular protected training list (at least 1x/week), and preferably provide a senior trainer; while the trainees recognise that it is expected they PA G E 7 attend. The excuse (by either the trainee or echo department) that there is no time to train is of great concern, and while we acknowledge departments are working under pressure the importance of training future cardiologists in this core skill cannot be emphasised enough. There are huge advantages in encouraging the presence of StR’s in the echo lab. More complex echo studies (e.g. contrast administration for LV opacification or agitated saline for assessment of a intracardiac shunt), as well as valuable dialogue between physiology and clinical teams is an essential when striving to deliver a quality service. Further, to facilitate better physiology engagement the BSE have suggested a regional physiology lead as a formalisation of their inclusion in the training process. This would create a dialogue and understanding between the two groups of the weaknesses and strengths in training within the region and how this might be addressed. 2. Greater flexibility in BSE TTE Accreditation process allowing a greater number to trainees to achieve this standard. Currently echocardiography competency for cardiology trainees is assessed through the following mechanisms: (i) knowledge based assessment exam undertaken at the ST3 stage of training and (ii) a practical competency assessment (table 1). Practical competency can be demonstrated either by completing BSE TTE accreditation or achieving 6 DOPS, completed by 2 different assessors. If trainees chose to use DOPS for assessment they are strongly encouraged to complete the BSE curriculum based assessment tool in order to provide evidence of experience across a breadth of cardiac pathologies. Data from the 2013 BJCA survey suggests that although many trainees wish to obtain BSE accreditation, the numbers actually achieving this are low (26% of all trainees surveyed). Trainees felt that the requirement for compiling a logbook in a 12 month period is too difficult to achieve. In addition not all departments may have the capacity to offer trainees the opportunity to attain BSE accreditation. In order to try and address this issues BSE have recently extended the time duration for collating a logbook to 24 months around the time of the examination; and this change has been active since October 2013. echocardiography competency in an appropriate time-frame It was interesting to note that during the Joint BSE/BJCA training day discussion, trainees did not have a clear understanding on the process in which they raised concerns regarding failure to progress in their echo training; indeed some feared negative repercussions if they did so. Currently concerns may be directed to either clinical or educational supervisors, training programme director or to the annual review of competence progression (ARCP) panel. The ARCP is the formal annual process by which a trainee’s progression is reviewed and assessed. Trainees reported that often echocardiography was not specifically asked about and when concerns were raised, they were not necessarily addressed. The appointment of an Echo director, has been advised by the Cardiology SAC (Chair Dr Ian Wilson). They would be responsible for ensuring the trainee had access to regular echo training lists, through acting as a point of contact for trainees to raise any concerns, addressing any issues raised and ensuring training is being delivered to individual trainees to a satisfactory level. Furthermore greater clarity of what trainees should practically expect from echocardiography training will also facilitate this. The key roles of individual stakeholders are summarised in table 2. 4. Concept of modular training One key aspect raised by the trainees was the need for early acquisition of hands-on echo skills. They were keen for StR entry-level focused training in echocardiography. Some trainees struggle to obtain the necessary standard in competency, which if reached to a desired level is acquired late in their training program. Hence the BJCA are very keen to see the establishment a modular type approach, where 1-3 months is spent training in an echo lab performing a high volume of transthoracic echo studies. This intense focused training will bring the StR up to speed rapidly, and usefully set the scene for further development of such skills; hugely benefiting the trainees and their patients, as well as other staff. However, in the current system this may not be feasible in all hospitals. Simulator training has been suggested as a useful adjunct and in the absence of modular training may help to partially bridge the gap. Although it is agreed that BSE accreditation (or its equivalent) should be mandatory for those who intend to pursue imaging subspecialty, not all trainees will need or want to undertake this formal process. However the alternative, of 6 DOPS, may not be robust enough to ensure proficiency in TTE. Given that much of the echo training delivered in the UK will be by physiologist they are not be familiar or trained in this form of assessments and there is a lack of clarity as to whether they can complete them. For those pursuing this alternative approach the BSE assessment tool in addition to an informal logbook may provide a more comprehensive approach. Therefore, a vital aspect of supporting such training is clarification of what exactly is meant by core echo training. Currently, a document on ‘Training Cardiologists in Echocardiography in the UK’ is under development, led by Dr Thomas Matthew, BSE Lead for Trainees. The BCS have run pilot courses in simulation training, centered on patient safety. This is proving to be very popular amongst trainees. The benefits of simulation training have been widely assessed in medicine and multiple articles exist in the literature. Simulator based medical education has been shown to be superior to the traditional didactic system of education 1-3. Six competencies are defined: patient care, medical knowledge, practice-based learning, interpersonal skills, professionalism and system based practice 4, 5. Simulation training has the potential to facilitate proficiency in all six areas and where appropriate allows re-creation of clinical scenarios helping standardize medical education and training. This improved proficiency leads to better patient care and management with improved patient outcomes 6, 7. There is no doubt that simulation based training accelerates learning 8. 3. Identifying and supporting trainees who are not achieving A number of echo simulator training systems exist1. The most popular in the UK is Heartworks1. Important features of this PA G E 8 system include programs in transthoracic and transoesophageal echocardiography, excellent anatomical virtual imaging along side echo images, and normal heart studies along with an increasingly wide range of cardiac pathologies. References • Shakil O, Mahmood F, Matyal R. Simulation in echocardiography: an ever-expanding frontier. J Cardiothorac Vasc Anesth. 2012 Jun;26(3): 476-85 BSE Initiative • Hartman GS, Christopher WW, Mullin M, et al: A virtual The BSE run a national course in echocardiography, Core Knowledge, which is lecture based and includes case reviews and discussions. As a direct result of the issues highlighted in echo training nationally, the BSE are in the process of devising a echo training course which will be aimed at all core cardiology trainees and will incorporate core knowledge lecture series and simulator training. The aim is to engage each training region to provide a regional simulation training centre(s), once the trainee has attended a 2 day lecture course. The advantages of regional engagement in this process are significant. Creating a forum for echo training and discussion, with the opportunity to meet the Echo Training Director. reality transesophageal echocardiography (TEE) simulator to facilitate under- standing of TEE scan planes. Anesthesiology 95: A545, 2001. • McGaghie WC, Issenberg SB, Cohen ER, et al: Does simulation- based medical education with deliberate practice yield better results than traditional clinical education? A metaanalytic comparative review of the evidence. Acad Med 86:706-711, 2011 • Eason MP: Simulation devices in cardiothoracic and vascular anesthesia. Semin Cardiothorac Vasc Anesth 9:309-323, 2005 Conclusion • Okuda Y, Bryson EO, DeMaria S Jr, et al: The utility of A change in the attitudes and delivery of echo training is long over due. There is raising momentum and a will to see this change for the better. By raising awareness of the issues and providing a clarity as to the responsibilities of each key player in this fight we will help accelerate the changes needed to achieve high quality echo training across the UK. Like the SAC and BCS, the BSE are committed to this and will continue to increase their efforts. Further national training days are planned; and under development are: a formal document offering guidance in echo training; a nationally delivered course with inclusion of simulator training; and greater emphasis given on issues specific to trainees at the annual BSE conference. As always the authors welcome any suggestions on how we can further these goals. Anna Kydd and Bushra Rana, Contributors: Thomas Mathew, Rick Steeds, Guy Lloyd (BSE) Rizwan Sarwar, Afzal Sohaib, David Holdsworth (BJCA) simulation in medical education: What is the evidence? Mt Sinai J Med 76:330-343, 2009 • Barsuk JH, Cohen ER, Feinglass J, et al: Use of simulationbased education to reduce catheter-related bloodstream infections. Arch Intern Med 169:1420-1423, 2009 • Draycott T, Sibanda T, Owen L, et al: Does training in obstetric emergencies improve neonatal outcome? Br J Obstet Gynaecol 113: 177-182, 2006 • Sharma V, Chamos C, Valencia O, Meineri M, Fletcher SN. The impact of internet and simulation-based training on transoesophageal echocardiography learning in anaesthetic trainees: a prospective randomised study. Anaesthesia. 2013 Jun;68(6):621-7 FRONT COVER Left ventricular pseudoaneurysm This image demonstrates a left ventricular pseudoaneurysm as a complication of a late presentation anterior ST elevation myocardial infarction. Left ventricular pseudoaneursyms are characterised by localised rupture of the myocardium contained by the pericardium and organised haematoma, with walls lacking in myocardial tissue. Due to the friable nature of their containment, LV pseudoaneuysms are prone to rupture, with often catastrophic consequences. Prompt identification and treatment (by surgical repair) is of upmost importance. Laura Dobson Monashheart, Melbourne, Australia PA G E 9 UNI TO QUINTI obstruction. The term sclerosis is now frowned upon as it is the forerunner of later organic degenerative valve dysfunction THE SPECTRUM OF AORTIC VALVES 2. Bicuspid. For many years aortic valve disease in adults was an acquired disorder. Little attention was paid to any other alternative, aortic valves were either normal, rheumatic or syphilitic. Both the latter have for practical purposes disappeared in the Western world, with age related degenerative diseases replacing them. However, aortic valve disease presenting in younger adults is, through the medium of available and quality non-invasive imaging, recognised frequently to be related to congenetal aortic valve pathology. Severe congenital conditions present in the newborn or in early infancy and generally are a different pathology or grade of severity to the congenital conditions which do not manifest themselves until late teenage or adult life. I will therefore be referring only to the adult presenting aortic valve disorders. 1. Tricuspid aortic valve Consider initially the descriptive terminology of the valve structure. a) Cusp. This strictly describes the edge or tip of a leaflet although the term is often used in the context of leaflet. A Bicuspid Aortic Valve (BAV) is the commonest congenital abnormality occurring in up to 2% of the general population with a predominance in males. Although seen relatively frequently in an echo department the condition often gives rise to questions of doubt or debate. The reason for this relates to the number of variations of bicuspid aortic valve structure. Here, terminology is important so that describing the image findings is essential to the correct image interpretation. The cusp, leaflet and commissural terms have already been mentioned but a fundamental additional term is: d) Raphe. This term is used to describe “fusion”. With underdeveloped leaflets, their edges are or can be fused together resulting in a thickened abnormal commissural ridge between the abnormal leaflets. This fusion of the two underdeveloped leaflets may result in them functioning together as a single leaflet . With the other unaffected leaflet the valve in effect functions as a two leaflet or bicuspid valve. A” pure”BAV will have two similarly sized leaflets with nothing fused, hence no raphe. Rather than the term” pure”, this variant has been termed type “ 0” (no raphe).The catagorisation refered to is that of Sievers et all 1. It should at this point be appreciated that there are a number of different catagorisations of BAVs with different terminology. b) Leaflet. This is the more appropriate term for the structural elements or components of the valve These terms can be used interchangeably e.g. tricuspid or tri leaflet, but traditionally the term cusp is the accepted descriptive term, describing the number of components to the valve i.e. bicuspid or tricuspid etc. A normal or tricuspid aortic valve (also known as a semilunar valve) has three equal edges of parallel cusp apposition. c) Commissure. This traditionally describes the free edge of a valve leaflet. Leaflet edges are in apposition when leaflets close. This article is not intended to describe aortic valve dysfunction. However, it is appropriate to discuss briefly age-related changes to an originally normal tricuspid aortic valve. This is in the context that such changes can result in imaging interpretation difficulties when considering whether or not a pathological valve was initially tricuspid or bicuspid. Another common situation is the so-called “ sclerotic”aortic valve in which there is some thickening and fibrosis of the leaflets and or commissure edges resulting in a flow murmur although the valve opens satisfactorily without causing measurable PA G E 10 The variant described above with the fusion of two small underdeveloped leaflets fused by one raphe has been termed1 (referring to one raphe) using the Sievers terminology. In addition to a raphe fusing the commissural edges of two underdeveloped cusps there may also (relatively rarely) be an additional raphe fusing one edge of one of the smaller leaflets to the leaflet edge of the one larger normal cusp. This results in 2 raphes and this variant has been termed a type 2 BAV. The simple diagram (figure 1) depicts these BAV variants. 0 raphes - Type 0 1 raphes - Type 1 2 raphes - Type 2 Fig. 1. Types 1 and 2 although having identifiable albeit two smaller leaflets, the fusion results in them being effectively only two functional leaflets. Type 1 is by far the commonest variant. Although bicuspid valves are structurally abnormal they generally function satisfactorily until the fibrous raphe and commissural edge thickening becomes more extensive resulting in restrictive valve opening, hence developing aortic stenosis. Stenosis is the commonest presentation albeit invariably with some regurgitation. To have regurgitation as the dominant functional defect occurs in less than a third of cases. The median age for requiring an aortic valve replacement is in the mid 30s, highlighting the importance of intermittent followup and reassessment once a BAV has been recognised (which is currently usually in childhood). Bicuspid valve’s are associated with a significant tendency to be accompanied by developing aortic root dilatation which may extend up to the aortic arch. Originally, when it was recognised that the aortic wall structure associated with BAV’s was “ thinner”than the normal three layered aortic wall there being a relative absence of the middle or median muscular layer, the term”cystic medial necrosis” was utilised. This phrase is still often used mainly by habit although the basis for the defect is genetic with variant phenotypical developmental abnormalities rather than a necrotic process. Although most cases of BAV are incidental or sporadic, it is also recognised that there may be a familial association in as many as 15% of close relatives. Expressing this another way, in one study of 30 families of patients with BAV they found 11 families (37%) had more than one first-degree relative with a BAV (Chan et al 2 ). Some genes have been identified in the inheritance of BAV one being NOTCH1 with others being more recently identified demonstrating genetic heterogenicity and complex inheritance. The practical relevance is that the aorta may well be involved and requires study and measurement at the time of each echo assessment for BAV as it is the “rate of change”of the aortic when the route dimensions on echo are reaching the point of concern a thoracic CT scan will be required to assess the ascending aorta and aortic arch for dilatation. Invariably, expect to find some, albeit slight, variation between the CT and Echo measurements of aortic dimensions due to technique differences. This should not be interpreted as an error but is to be expected. It should be appreciated that aortic root dilatation is a distinct entity and is not dependant on the degree of aortic valve dysfunction. Given that a BAV is associated with aortic pathology , it is not surprising that aortic pathology further round the aortic arch, namely a coarctation of the aorta is also a common associated defect accompanying a BAV. Hence, interrogation of the descending thoracic aorta for evidence for or exclusion of coarctation is a mandatory requirement for an echo study involving a BAV. Any structural cardiovascular defect resulting in a surface irregularity of the endothelial lining of a heart valve is a potential site for bacteria to settle resulting in endocarditis. BAV is no exception with endocarditis being relatively common. Finally, when recognising a BAV on Echo, if it is of the pure type (type 0 ) with two cusps and no raphe the cusp apposition line can be lateral or antero- posterior. The common type of BAV ,type 1, with fusion of two smaller cusps with one larger cusp with one central raphe the direction of the effective two cusps is rarely anteroposterior and more often latero- lateral with the raphe aligned with the centre or middle of the greater cusp. When the closure line is latero- lateral, the right coronary artery usually originates from the right sinus of Valsalva and the left main stem from the left sinus. When the BAV’s orientated Bicuspid aortic valve Commissure Single cusp Raphe Conjoined cusp Fig. 2. Drawing of a BAV looking down from the aorta demonstrating one normal cusp with 2 cusps fused by a fibrous "raphe". The coronary ostea are apparent. root dimensions rather than the absolute values which direct the timing of surgery for an aortic root replacement. To assess how much of the ascending aorta and aortic arch may be involved, Fig. 3. A bicuspid valve at the time of surgery with the arrow highlighting the raphe. with the closure line antero posterior both coronary arteries may have a common origin from the anterior sinus. Rarely this has been reported to be associated with sudden cardiac death during exercise. Hence, without propagating alarm it is appropriate to report the orientation of the valve in the Echo report. PA G E 11 TOE examination, some not being recognised until surgical excision. Bicuspid valves are well known to have an increased association with aortic dissection but unicuspid valves even more so. In an autopsy study of 161 cases of aortic dissection the risk of dissection associated with a bicuspid valve was 9 times and with a unicuspid valve 18 times that of subjects with a tricuspid aortic valve ( Larson et al 4). Emphasis therefore is Type 0 (No Raphe) 20% 9% Type 1 Type 2 (One Raphe) (Two Raphes) 59% 10% 2% Fig. 4. Frequency of distribution of BAV types. 3)Unicusp The presence of only one aortic valve cusp was for many years only detected either at surgery for an aortic valve replacement or as an incidental post-mortem finding. Echocardiography change that with reports of recognition initially in childhood but but now occurring as adult case reports (Krishnamoorthy 3) Presumably, as with by bicuspid valve leaflets which are structurally abnormal, the single cusp of a unicuspid valve thickens and becomes fibrotic at a much earlier age than normal tricuspid valve cusps. Hence presentation with aortic stenosis has been the consistent clinical presentation. The time of presentation is in early adult life with approximately 50% of cases reported requiring an AVR in their mid 30s. A degree of aortic regurgitation invariably coexists. The other notable feature, again similar to bicuspid aortic valves is the predominance of males and a strong association with dilatation of the ascending aorta. The incidence of unicuspid aortic valves is low and reported to be between 0.9% and 6% in various series of patients undergoing aortic valve replacement. The mechanism of function of a unicuspid valve is generally that of the single cusp being attached posteriorly between the usual position of the non and left coronary cusps. Occasionally some valves are described as having or being a single membrane like leaflet with a central valvular orifice. Most however are leaflet like having an eccentric opening area along its free edge opposite its side of attachment. Distinguishing this on echo from a bicuspid valve which is functionally unicuspid i.e. a”pseudo”unicuspid valve from fusion, fibrosis or calcification of one of the two bicuspid valve leaflets can be difficult at best or impossible even on a Fig. 5. Diagramatic illustration of a unicuspid aortic valve. PA G E 12 Fig. 6. A short axis parasternal view of a BAV in diastole. The 2 fused cusps are of different size. Fig. 7. A bicuspid aortic valve with 2 equal sized aortic leaflets Fig. 8. A bicuspid valve withone raphe illustrating early calcification of the 2 abnormal leaflets on recognition, measurement and trends of progression of the ascending aorta in unusually looking aortic valves which may be bi or unicuspid. 4) Quadricuspid. Quadricuspid aortic valves, recognised as incidental findings have been published as case reports in previous editions of Echo. They are reported to be rarer than unicuspid aortic valves. In terms of quadricuspid semi-lunar valves, quadricuspid pulmonary valves are reported to be nine times more common than quadricuspid aortic valves. A quadricuspid pulmonary valve almost always appears to function normally and generally are detected incidentally at post-mortem. Quadricuspid aortic The coronary ostea may be misplaced and cause surgical problems at the time of an aortic valve replacement. There has been at least one case report of sudden death in a teenager due to coverage of the left coronary ostea by leaflet tissue in a quadrant has valve. Interestingly the quadricuspid aortic valve is not reported to be associated with developing aortic root or ascending aortic abnormality and only rarely are quadricuspid valves reported to be a site for endocarditis. Although patients with a BAV not uncommonly also have a bicuspid pulmonary valve it is interesting that no patients have been reported to have simultaneously both a quadricuspid aortic and pulmonary valve. 5) Quinticuspid. To have 5 aortic valve cusps is very rare with to date only three case reports of this anomaly (Bogers et al 5). Therefore, although unlikely, it is always worth keeping an eye open for. The variants of human anatomy continue to be ever fascinating. Gordon Williams Editor References Fig. 9. A quadricuspid aortic valve with 4 equally sized cusps imaged in diastole 1. A classification system for the bicuspid aortic valve from 304 surgigal specimens. Sievers H-H and Schmidtke C J Thoracic Cardiovasc Surg 2007;133:1226 2. A prospective study to assess the frequency of familial clustering of congenital bicuspid aortic valve. Huntington K, Hunter AG, Chan KL J Am Coll Cardiol, 1997; 30, 1809 3. Images in Cardiology: Unicuspid aortic valve Krishnamoorthy KM Heart 2001; 85:217 Fig. 10. The same valve as fig 9 seen in systole with the 4 equally sized leaflets fully open. valves, presumably because of their high pressure environment do become dysfunctional in adult life predominantly with incompetence with the requirement for an aortic valve replacement being slightly later in age than for a bicuspid valve. The valve structure of a quadricuspid aortic valve is generally that of three equal sized cusps and one smaller cusp, the next most frequent combination being 2 equal sized larger cusps and 2 equal smaller ones and finally just 4 equal sized cusps. Again, these quadricuspid valves occur more commonly in males. 4. Risk factors for aortic dissection: a necropsy study of 161 cases. Larsen EW, Edwards WD Am J Cardiol 1984;53:849 5. Quinticuspid aortic valve causing incompetence and stenosis Bogers AJJC, Zulfukar A, Hendriks FFA, Huysmans HA Thorax 1982;37:542 PA G E 13 NEW GUIDELINES A guideline protocol for the assessment of restrictive cardiomyopathy Lead Authors Dr. D. Knight, Dr. K. Patel, Dr. C. Whelan Education Committee Authors Dr Rick Steeds (Chair), Will Bradlow, Alison Carr, Richard Jones, Prathap Kanagala, Daniel Knight, Guy Lloyd, Thomas Mathew, Navroz Masani, Kevin O’Gallagher, David Oxborough, Bushra Rana, Liam Ring, Julie Sandoval, Martin Stout, Gill Wharton, Richard Wheeler 1. Introduction 1.1 The BSE Education Committee has published a minimum dataset for a standard adult transthoracic echocardiogram, available on-line at www.bsecho.org. This document specifically states that the minimum dataset is usually only sufficient when the echocardiographic study is entirely normal. The aim of the Education Committee is to publish a series of appendices to cover specific pathologies to support this minimum dataset. 1.2 The intended benefits of such supplementary recommendations are to: • Support cardiologists and echocardiographers to develop local protocols and quality control programs for adult transthoracic study; • Promote quality by defining a set of descriptive terms and measurements, in conjunction with a systematic approach to performing and reporting a study in specific disease-states; • Facilitate the accurate comparison of serial echocardiograms performed in patients at the same or different sites. 1.3 Understanding restrictive cardiomyopathy (RCM). This document gives recommendations for the image and analysis dataset required in patients being assessed for restrictive cardiomyopathy (RCM). RCM is a functional classification that is made on the basis of adverse filling of the left ventricle and is therefore different from the structural changes that describe other forms of cardiomyopathy (such as hypertrophic or dilated). RCM can either be primary or more commonly secondary to various conditions (see table) adversely affecting the filling pattern of the left ventricle. The natural histories of conditions causing myocardial restriction exhibit a spectrum of cardiac pathophysiology from subclinical (including the early stages of diastolic dysfunction) through to severely restrictive diastolic filling patterns. Thus the operator should take care to interpret more subtle findings that may be the only manifestations of disease development, with novel deformation imaging assisting in the identification of early disease states. The morphological and anatomical features of causative pathologies in RCM can be indicative but not specific of an underlying disease state. The majority of RCMs are secondary to systemic aetiologies, the commonest of which is amyloidosis. In contrast, idiopathic (primary) RCM is rare. The term amyloidosis describes a group of disorders caused by abnormal folding, aggregation and accumulation of certain proteins in the tissues, in an abnormal form known as amyloid deposits. This document gives recommendations for the image and analysis dataset required in patients being assessed for RCM with a particular reference to cardiac amyloidosis and the transthoracic echocardiography protocol performed at The UK National Amyloidosis Centre (NAC), with whom this guideline has been co-authored (http://www.ucl.ac.uk/medicine/amyloidosis). While echocardiography allows a comprehensive assessment in RCM, it is important to remember the complementary role of other imaging modalities, including cardiac MRI. Primary Idiopathic Secondary Infiltrative disorders • Amyloidosis • AL: cardiac involvement common. • Transthyretin (ATTR): familial variant, usually autosomal dominant. • Age-related: senile in 25% aged > 80 years (Wild Type ATTR); atrial in 90% aged > 90 years (deposits derived from atrial natriuretic peptide, ANP). • AA: cardiac involvement rare. • Haemosiderosis (for example: haemochromatosis, transfusion-related iron overload) • Sarcoidosis Endomyocardial fibroelastosis Scleroderma Radiotherapy Adapted from Nihoyannopoulos & Dawson, European Journal of Echocardiography PA G E 14 (2009) 10, iii23–iii33 1.4 The distinction between concentric remodeling versus concentric hypertrophy (see figure) is an important concept that is poorly understood, but is of prognostic significance in patients with preserved left ventricular ejection fraction. The distinction requires the calculation of relative wall thickness (RWT) and LV mass using the following formulae: RWT = (2 x LVPWd) ÷ LVIDd LV mass = 0.8 x {1.04 x [(LVIDd + LVPWd + IVSd)3 - (LVIDd)3]} + 0.6 g Where LVIDd = left ventricular internal dimension in diastole, LVPWd = left ventricular posterior wall width in diastole, IVSd = interventricular septal width in diastole. RWT is increased (≥ 0.42) in both concentric remodeling and hypertrophy, but in infiltrative cardiomyopathy the important distinction is the increased left ventricular mass (>95 g/m2 in females, >115 g/m2 in males). Conversely, the measurement of RWT in cases of increased LV mass allows the distinction between concentric (relative wall thickness ≥ 0.42) and eccentric (< 0.42) hypertrophy. 1.5 The views and measurements are focused upon RCM and are supplementary to those outlined in the minimum dataset. These are given assuming a full study will be performed in all patients. 1.6 When the condition or acoustic windows of the patient prevent the acquisition of one or more components of the supplementary Dataset, or when measurements result in misleading information (e.g. off-axis measurements) this should be stated. 1.7 This document is a guideline for echocardiography in the assessment of RCM and will be up-dated in accordance with changes directed by publications or changes in practice. 2. List of abbreviations 2.1 Views: PLAX A4C A5C SSN parasternal long axis apical four chamber apical five chamber suprasternal PSAX A2 C SC ALAX parasternal short axis apical two chamber subcostal apical long axis or apical three chamber PW pulse wave Doppler CW continuous wave Doppler CFM colour Doppler TDI tissue Doppler imaging LA AV LVOT RA RVOT RL/RU/LL/LU PV IVC LVIDd/s LVPWd RVd RWMA MAPSE left atrium aortic valve left ventricular outflow tract right atrium right ventricular outflow tract right lower/right upper/left lower/left upper pulmonary vein inferior vena cava left ventricular internal dimension in diastole/systole left ventricular posterior wall width in diastole right ventricular cavity diameter in diastole regional wall motion abnormality mitral annular plane systolic excursion 2.2 Modality: 2.3 Measurement and explanatory text: LV MV Ao RV PV L/R PA TV STJ IVSd/s PHT VTI TAPSE left ventricle mitral valve aorta right ventricle pulmonary valve left/right pulmonary artery tricuspid valve sinotubular junction interventricular septal width in diastole/systole pressure half-time velocity time integral tricuspid annular plane systolic excursion A ‘*’ indicates that these findings, particularly when found together within an individual echo study, are strongly suggestive of cardiac amyloidosis PA G E 15 VIEW Modality Measurements Explanatory note for ARVC PLAX 2D/Mmode LV dimensions (LVIDs, LVIDd) LV cavity size may be normal or small LV wall thickness (IVSd, LVPWd) May be normal If > 12 mm concentric thickening in the absence of other pathology (for example, hypertension, HCM or significant aortic stenosis) may suggest infiltrative disease Note: AL Amyloidosis particularly causes LV increased wall thickness in the mild to moderate range whereas TTR causes LV increased wall thickness in the moderate to severe range (although there is overlap) LV mass LV mass = 0.8 x {1.04 x [(LVIDd + LVPWd + IVSd)3 - (LVIDd)3]} + 0.6 g Care should be taken to ensure accurate 2D measurements, as errors are amplified by cubing when calculating LV mass Relative wall thickness Relative wall thickness = (2 x LVPWd) ÷ LVIDd In infiltrative cardiomyopathy there is concentric hypertrophy *Granular or speckled appearance of myocardium Although this feature is known to be a characteristic feature of cardiac amyloidosis, it is not a specific finding and hence should not be used in isolation Note: Low dynamic range, low grey scale compression and harmonic imaging can mimic this appearance. Turning off ‘harmonic’ settings may help to reduce over diagnosis *Aortic and mitral valve leaflet thickening Homogenous thickening of leaflets of all valves often seen in amyloidosis Note: Caution should be taken in this qualitative assessment when using harmonic imaging, which may give rise to the appearance of valve leaflet thickening (see note above) PSAX 2D *Pericardial and pleural effusions Frequently, trace or small pericardial and pleural effusions are seen LV wall thickness at 4 points using clock face as reference (12, 3, 6, 9) 2D frozen image at mid LV level at end diastole to demonstrate concentric increased wall thickness Note: Avoid inclusion of papillary muscles when measuring LV wall thickness by 2D caliper PA G E 16 Image Apical 4CH Apical 4CH and 2 CH 2D 2D EF (Simpson’s Biplane) Reduced in end stages, but may be normal or mildly reduced in early disease *IAS thickening Visual assessment *Mitral and tricuspid valve leaflet thickening Visual assessment: homogenous thickening RA and LA volumes and areas Measured at end ventricular systole and BSA indexed Biatrial dilatation: RA area> 19cm_, LA volume>28ml/m_ Apical 4CH M-mode MAPSE MAPSE<10mm Reduced longitudinal function may be seen before deterioration in global function assessed by EF Apical 4CH PW Doppler MV inflow pattern: E/A ratio Severe diastolic dysfunction is more suggestive of an underlying restrictive cardiomyopathy. Earlier in the natural history of restrictive disease, abnormalities of LV filling by PW Doppler of mitral inflow may be in the mild or moderate categories of diastolic dysfunction. Please refer to the BSE diastolic function assessment guidelines E deceleration time Short deceleration time. Note: normal diastolic filling is extremely rare in cardiac amyloidosis Mitral annulus: In restrictive filling: e’ Restrictive filling pattern with low e’ e’/ a’ e’/ a’ << 1 E/e’ Sept and Lat E/e’ (average of septal and lateral mitral annulus) > 13 Apical 4CH PW TDI Earlier in the natural history of restrictive disease, abnormalities of mitral annular PW TDI may be in the mild or moderate categories of diastolic dysfunction. Please refer to the BSE diastolic function assessment guidelines PA G E 17 s’ Reduced systolic velocity. Reductions in TDI systolic and diastolic indices typically occur earlier in the natural history of the amyloid disease process than traditional echocardiographic measures, and may be a subclinical marker when this condition is suspected Apical 4CH PW Doppler PV flow: PVs/PVd PVa adur - Adur In restrictive filling: PVs << PVd ≥ 0.35 m/s ≥ 20 ms Apical 5CH PW or CW Doppler IVRT Short IVRT (<50ms) is in keeping with severe restrictive filling, but in earlier stages of the disease process may be prolonged or pseudonormal. Please refer to the BSE diastolic function assessment guidelines IVRT is quantified as the time interval between the end of LVOT ejection and the onset of mitral inflow. This can be quantified by PW or CW Doppler to record both mitral inflow and LVOT outflow velocity profiles: - PW Doppler: position the sample volume within the LVOT, but in close proximity to the anterior mitral valve leaflet - CW Doppler: position the Doppler beam in a hybrid position that captures mitral inflow and LVOT outflow Subcostal 2D RV free wall thickness M-mode M-mode or 2D frozen image with zoom at end-diastole at the level of the tricuspid valve chordae tendinae ≥ 5 mm RV free wall thickening is abnormal and is frequently seen in cardiac amyloidosis The administration of intravenous agitated saline may assist in situations where endocardial definition is poor PA G E 18 Apical 4CH and 2Ch Deforma Global and peak longition tudinal systolic strain imaging (optional but extremely useful) Reduced with relative apical sparing, giving rise to a characteristic ‘bull’s eye’ appearance on speckle tracking software* Ensure high quality, optimized views for speckle tracking post-processing. This should result in a frame rate that is commensurate with optimal speckle tracking (at least > 80 fps) Reductions in strain indices typically occur earlier in the natural history of the amyloid disease process than traditional echocardiographic measures, and may be a subclinical marker when this condition is suspected Due to inter-vendor variability, ‘cut-off’ values are not currently advised, but must be interpreted relative to normative data for individual speckle tracking packages References 1. Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, et al. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008;29:270-6. 2. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440-63. 3. Nihoyannopoulos P, Dawson D. Restrictive cardiomyopathies. European journal of echocardiography : the journal of the Working Group on Echocardiography of the European Society of Cardiology. 2009;10:iii23-33. 4. Quinones MA, Otto CM, Stoddard M, Waggoner A, Zoghbi WA. Recommendations for quantification of Doppler echocardiography: a report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. J Am Soc Echocardiogr. 2002;15:167-84. Further reading about cardiac amyloidosis and evidence for novel techniques for assessing myocardial function 1. Banypersad SM, Moon JC, Whelan C, Hawkins PN, Wechalekar AD. Updates in cardiac amyloidosis: a review. Journal of the American Heart Association. 2012;1:e000364. 2. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. The American journal of cardiology. 1986;57:450-8. 3. Dungu JN, Anderson LJ, Whelan CJ, Hawkins PN. Cardiac transthyretin amyloidosis. Heart. 2012;98:1546-54. 4. Hu K, Liu D, Herrmann S, Niemann M, Gaudron PD, Voelker W, et al. Clinical implication of mitral annular plane systolic excursion for patients with cardiovascular disease. European heart journal cardiovascular Imaging. 2013;14:205-12. 5. Koyama J, Ray-Sequin PA, Falk RH. Longitudinal myocardial function assessed by tissue velocity, strain, and strain rate tissue Doppler echocardiography in patients with AL (primary) cardiac amyloidosis. Circulation. 2003;107:2446-52. 6. Milani RV, Lavie CJ, Mehra MR, Ventura HO, Kurtz JD, Messerli FH. Left ventricular geometry and survival in patients with normal left ventricular ejection fraction. The American journal of cardiology. 2006;97:959-63. 7. Phelan D, Collier P, Thavendiranathan P, Popovic ZB, Hanna M, Plana JC, et al. Relative apical sparing of longitudinal strain using two-dimensional speckle-tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis. Heart. 2012;98:1442-8. 8. Pinney JH, Whelan CJ, Petrie A, Dungu J, Banypersad SM, Sattianayagam P, et al. Senile systemic amyloidosis: clinical features at presentation and outcome. Journal of the American Heart Association. 2013;2:e000098. 9. Rahman JE, Helou EF, Gelzer-Bell R, Thompson RE, Kuo C, Rodriguez ER, et al. Noninvasive diagnosis of biopsy-proven cardiac amyloidosis. Journal of the American College of Cardiology. 2004;43:410-5. PA G E 19 10. Rapezzi C, Merlini G, Quarta CC, Riva L, Longhi S, Leone O, et al. Systemic cardiac amyloidoses: disease profiles and clinical courses of the 3 main types. Circulation. 2009;120:1203-12. 11. Rapezzi C, Quarta CC, Riva L, Longhi S, Gallelli I, Lorenzini M, et al. Transthyretin-related amyloidoses and the heart: a clinical overview. Nature reviews Cardiology. 2010;7:398-408. 12. Selvanayagam JB, Hawkins PN, Paul B, Myerson SG, Neubauer S. Evaluation and management of the cardiac amyloidosis. Journal of the American College of Cardiology. 2007;50:2101-10. 13. Wenzelburger FW, Tan YT, Choudhary FJ, Lee ES, Leyva F, Sanderson JE. Mitral annular plane systolic excursion on exercise: a simple diagnostic tool for heart failure with preserved ejection fraction. European journal of heart failure. 2011;13:953-60. Letters to the Editor To enhance ECHO both for the authors of submissions and for other readers, if you have any views regarding items appearing in ECHO please write to the editor. Publishing your views and comments, inviting responses from authors and readers can make ECHO an even more enjoyable and informative publication. P leas e email t he edit or at : [email protected] PA G E 20 CASE REPORTS 1) Late presentation Marfan’s syndrome A 33 year old Caucasian male was admitted with a 4 week history of sporadic severe chest pain which was exacerbated with anterior movement. He had a 2 month history of, persistent cough, SOB and was diagnosed with bilateral pneumonia and hypertension. This patient also had a high occurrence of self discharge. His long term history divulged an ocular lens dislocation aged 4 and a spinal malformation diagnosed aged 13. At this admission his 12 lead ECG revealed Sinus tachycardia (105 bpm) with RBBB. Auscultation yielded an apex to right jugular ESM with chest X- ray indicating cardiomegally leading to a 2D TTE referral for: Collapsing pulse ?Severe AR/dissection. Fig. 2. Subcostal view with focus on abdominal aorta highlighting extent of the dissection. fragmentation, myxoid change and dissection. This histopathological analysis pinpoints Marfan’s syndrome as the causative factor of the cardiac abnormalities noted. Following uneventful post surgical recovery the patient was discharged 7 days later. A subsequent 5 month follow up 2D TTE performed at the tertiary centre demonstrated a notable improvement in cardiac status showing good left ventricular systolic contractility with normal cavity size and mild concentric hypertrophy. The bi-leaflet mechanical aortic prosthesis was well seated with trivial “washing jet” regurgitation. Ascending aorta and arch were normal in size with dilated descending aorta as previously noted pre surgery. Discussion Fig. 1. PLAX view highlighting dilated aorta with poor AV coaptation and intimal tear (dissection). Portable, bedside, 2D TTE demonstrated a severely dilated aortic root measuring; 8cm (Figure: 1) with associated malcoaptation of the aortic valve leading to severe free flowing aortic regurgitation (AR PHT = 133ms). A sub acute type: A dissection was evident with a prominent dissection flap with independent movement and an associated false lumen noted in numerous views. The ascending and descending aorta were also severely dilated with the associated dissection being noted in the suprasternal (Figure: 2) and subcostal views (Figure: 3) highlighting the length and severity of the intimal tear throughout the aorta. Marfan syndrome is a systemic disorder of connective tissue caused by mutations in the extracellular matrix protein fibrillin 1 with a UK incidence of 2-3 per 10,000 individuals2. It is a multisystem disorder occurring worldwide with no predilection for either sex with manifestations typically involving the cardiovascular, skeletal and ocular systems. Cardiac manifestations within the heart are confined to thickening and/or prolapse of both the mitral and/or tricuspid valve and aortic valve dysfunction3. This is generally a late occurrence, attributed to stretching of the aortic annulus by an expanding root aneurysm. The left ventricle was severely dilated (LVIDd = 7.3cm) due to the longevity of the undiagnosed severe aortic regurgitation with moderately impaired systolic contractility (EF = 42%) as a by-product of the low flow coronary perfusion attributed to the dilated sinus of valsalva and consequent malcoaptation of the aortic cusps. The patient was transferred to a local tertiary centre for aortic root, ascending aorta and hemi-arch replacement that was completed within 24 hours following diagnosis. Subsequent histological analysis of the native tissue, the aortic valve showed myxoid change and focal fibrosis. Ascending aorta histology showed medial degeneration, elastin Fig. 3. Suprasternal view of aortic dissection initmal tear. PA G E 21 Marfan accounts for the majority of cases of aortic dissection in < 40 year olds. The diagnosis of aortic dissection has been missed in up to 30% of patients on initial evaluation, and in up to 28% of patients the diagnosis has been first established at post mortem examination3. Marfan syndrome mortality from complications of aortic root dilatation has decreased (70% in 1972, 48% in 1995) and life expectancy has increased (mean ± SD) age at death 32 ± 16 years in 1972 versus 45 ± 17 years in 19981. 2D TTE is the favoured modality in routine follow up of Marfan patients, with CT angiography and MRI providing more accurate images of the proximal aorta and are commonly utilised. The sensitivity and specificity of 2D TTE for the detection of aortic dissection range from 35 to 80% and 39 to 96%, respectively depending on the anatomic location of the dissection3. Conclusion It is poignant to highlight the late diagnosis of Marfan’s syndrome in this case due to the patient’s high incidence of self discharge in addition to the severity of the aortic intimal tear and its ability to be viewed via the images obtained in the standard 2D TTE BSE protocol. The post surgery 2D TTE highlights the ability of the heart to convalesce following significant trauma and to return to near normal size and function. No additional follow up imaging is available as this patient has continued to fail to attend many outpatient clinic appointments. Jonathan Eldridge, Alison Carr, Chris Gale Pinderfields general hospital References 1. Gray JR., Bridges AB et al. Life expectancy in British Marfan syndrome populations. Clinical Genetics. 1998, 54, pp. 124–8. 2. Judge, D.P., Dietz, H.C. Marfan’s syndrome. Lancet. 2005. 366 (9501), pp. 1965-1976. 3. Khan, I.A., Nair, C.K. Clinical, diagnostic and management perspectives of aortic dissection. Chest journal. 2002. 122 (1). 2) Percutaneous closure of aortic paravalvular regurgitation under transoesophageal echocardiography (2D and 3D) guidance Paravalvular regurgitation is an uncommon complication of aortic valve replacement. Clinical consequences are heart failure, arrhythmias and haemolysis. The risk of a re-do operation, which usually involves replacement of the dehiscence valve, carries a significant risk, especially in patients who have also undergone CABG. Percutaneous approach using vascular plug (Fig. 1) is a new promising technique. We describe a case of percutaneous closure of severe paravalvularaortic regurgitation, in a 65 years old male patient. He underwent an aortic valve replacement with a bioprosthetic valve and triple Fig. 1. PA G E 22 Fig. 2. Fig. 3. coronary artery bypass surgery 3 years ago. He presented to the cardiology clinic with heart failure symptoms. TTE and TOE (Fig. 2) and aortography (Fig. 3) confirmed severe paravalvular aortic regurgitation. According to EUROSCORE 2 model, the risk of a second surgical approach was significantly high ( ~5% risk of death). Therefore a percutaneous closure using Amplatzer vascular plug III was proposed. The procedure was Fig. 6. Fig. 4. Fig. 5. performed under general anaesthesia with fluoroscopy and TOE guidance.The role of echocardiography (TOE) 2D and 3D was important in guiding the operator during the procedure and to confirm optimal deployment (Figs. 4, 5) minimising possible complications. The degree of regurgitation was remarkably reduced as demonstrated by TOE (Fig. 6) and fluoroscopy (Fig. 7). The improvement in the clinical status was also significant ( from NYHA class 3 to class 1). Percutaneous closure of paravalvular leaks using vascular plug is a new technique which avoiding the risk ofrepeat surgery and reducing the hospital stay. Transoesophageal echocardiography has a pivotal role during the procedure. Fig. 7. C. Voukalis, M. Been, V. Dhakshinamurthy, D. Hildick-Smith University Hospital of Coventry and Warwickshire 3) AcuNav V intra-catheter echo in the role of transcatheter aortic valve implantation (TAVI) Interventional centres have adopted 2D and 3D intracardiac echocardiography (ICE, using Acunav V) in preference to transoesophageal echocardiography to guide different percutaneous procedures such as patent foramen ovale (PFO) closure, left atrial appendage and transcatheter aortic valve implantation (TAVI). One of the advantages of ICE is that there is no need for the use of general anaesthesia facilitating earlier hospital discharge, and obtaining a superior imaging capability. 1, 2 The preferred treatment for severe symptomatic aortic valve Figure A: CW Doppler ~ 5 m/s, 100mmHg PA G E 23 Figure D: TAVI device positioning Figure B: Heavily calcified aortic valve reduced ultrasound catheter manipulation during the procedure by a single operator was noted. RT3D ICE images of the device attached to the delivery catheter immediately prior to release (figure D) and following successful deployment (figure1D) are shown. Post procedure the patient recuperated successfully with decreased gradients across the aorta and an improvement in symptoms. In this case TAVI guided by ICE demonstrated that the procedure could be done faster, requiring only local anaesthesia and enabling an early hospital discharge. Furthermore, due to the capabilities of real time monitoring, less need for fluoroscopy and contrast agents. Alejandro Rendon S, Imperial College London Acknowledgments Figure C: PLAX AO valve in 3D stenosis is conventional aortic valve replacement. This involves open-heart surgery to replace the narrowed valve with a new artificial one. Transcatheter aortic valve implantation (TAVI) is an alternative option for patients with severe aortic stenosis (AS) who are classified as high-risk patients or patients not eligible for conventional aortic valve surgery. Quality of life is a critical measure of success for TAVI in this patient population. Two major studies paved the way to the increasing clinical use of TAVI. 3. 4 The first TAVI procedure in the UK, guided by ICE was done at the Royal Manchester hospital. A 78 year old male patient with severe aortic stenosis and breathlessness underwent a transfemoral TAVI procedure (figure A and B demonstrating CW Doppler and aortic valve by 2D AcuNav). A retrograde system delivery was introduced through the femoral artery allowing positioning of the prosthetic valve within the native stenotic aortic valve. The procedure was guided using an ACUSON AcuNav 3D ultrasound catheter (Siemens AG, Germany). The AcuNav V catheter was inserted via a second right femoral vein puncture providing real time three dimensional monitoring. RT3D ICE (figure C) allowed enhanced anatomical characterization of the narrow valve. A PA G E 24 Dr Vaikom S Mahadevan, Simon A Hampshaw, and all the staff at the Department of Cardiology, Manchester Heart Centre, Manchester Royal Infirmary, Manchester, UK References 1. Newton JD, Mitchell AR, Wilson N, et al. Intracardiac echocardiography for patent foramen ovale closure: justification of routine use. JACC. Cardiovasc Interv 2009;2:369; author reply 69–70. 2. Koenig P, Cao QL. Echocardiographic guidance of transcatheter closure of atrial septal defects: is intracardiac echocardiography better than transesophageal echocardiography? Pediatr Cardiol 2005;26:135–9. 3. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–607. http://dx.doi.org/10.1056/NEJMoa1008232. 4. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–98. http://dx.doi.org/10.1056/NEJMoa1103510. 4) Providing a Definitive answer; the use of Definity Transpulmonary contrast in the diagnosis of aortic dissection Contrast CT, MRI and trans-oesophageal echocardiography (TOE) have long been considered the gold standard for the diagnosis of Type A aortic dissection, however, alternative methods of diagnosis can sometimes be considered, especially in the patient too unwell to be transferred to the CT scanner or where there is a delay to intubation required to perform a transoesophageal echocardiogram. We report two cases where the use of Definity trans-pulmonary contrast with bedside transthoracic echocardiography (TTE) has led to a timely diagnosis of this often catastrophic condition. returned for a repeat echocardiogram 3 weeks later (Image B), with the impression of a dissection flap. Definity contrast injection confirmed the presence of a dissection flap, with contrast entering the true lumen and then the false lumen via the entry point of the dissection flap (Image C). A CT aortogram confirmed the presence of a type A aortic dissection (Image D). Case two An 83 year old female with a past history of atrial fibrillation and abdominal aortic aneurysm repair presented with abdominal pain and collapse to the Emergency Department. Initial CT Case one A 68 year old male was admitted with chest pain and raised inflammatory markers. An echocardiogram on admission revealed a moderate pericardial effusion (Image A) without clinical or echocardiographic evidence of cardiac tamponade. A diagnosis of acute pericarditis was made and he was discharged with a short course of colchicine with plans for surveillance out-patient trans-thoracic echocardiography. An unusual appearance of the ascending aorta was noted when he Image C Image A Image D abdomen revealed no overt intra-abdominal pathology, however, a large pericardial effusion was noted (Image E) and an urgent bedside TTE was performed. This confirmed a large pericardial effusion with echocardiographic features of cardiac tamponade including a fixed dilated inferior vena cava and diastolic compression of the right ventricle. The pericardial fluid had a homogenous echotexture suggestive of blood (Image F). Modified parasternal aortic views visualising the ascending aorta in short axis were suggestive but not diagnostic of aortic dissection. The administration of Definity confirmed the presence of a dissection flap in the proximal ascending aorta (Image G). Image B Aortic dissection is a relatively rare cause of chest pain, however, a missed diagnosis can have disastrous consequences and early diagnosis can be life-saving. Acute aortic dissection can be defined as a breach of the aortic intima leading to an intimal flap and passage of blood down a true and false lumen and usually occurs at a site of aneurysmal dilatation of the PA G E 25 Image E aorta. The dissection can spread from the site of the tear in an antegrade or retrograde fashion. Aortic dissection is associated with hypertension, dilatation of the aorta, collagen disorders (eg Marfans and Ehlers-Danlos), vasculitis, trauma and bicuspid aortic valve. It can be classified using the Stanford classification system as Type A (involving the ascending aorta and/or the aortic arch) or Type B (involving the descending aorta distal to the left subclavian artery without involvement of the ascending aorta). Patients presenting with type A dissection are often in extremis and without urgent surgical intervention are unlikely to survive. Type A dissection is frequently complicated by aortic regurgitation, cardiac tamponade, myocardial ischaemia (most commonly affecting the right coronary artery territory), haemothorax and acute neurological deficit. Diagnosis is often achieved by CT aortography (requiring the use of iodinated contrast), magnetic resonance imaging or trans-oesophageal echocardiography (requiring general anaesthetic). Patients can be too unstable to be transferred to the CT scanner and although near patient tests such as chest X-ray (widened mediastinum), blood pressure differential between the arms and D-dimer blood test can be helpful, none of these provide a definitive diagnosis. The sensitivity for the diagnosis of aortic dissection by TTE is poor (59.3%), mainly due to false positive findings in the ascending aorta 1 and therefore although it is often considered helpful in diagnosing the complications of dissection (tamponade, regional wall motion abnormalities, aortic regurgitation), it is not routinely used as a first line test for the assessment of the aorta. Transpulmonary contrast agents consist of microbubbles with thin and relatively permeable shells filled with high-molecular weight gas. The small size of the bubbles facilitates passage from the venous to the arterial system. The ability of ultrasound to detect these microbubbles relies on the unique non-linear behaviour of the bubble in the echo field, undergoing resonant oscillation in response to the variations in acoustic pressure transmitted by the transducer2. Contrast enhancement has been shown to be useful in transthoracic examinations when aortic dissection is suspected and the intimal flap is difficult to visualise or there is uncertainty in distinguishing a flap from an artefact3. It can also be helpful in distinguishing the true and false lumens. The true lumen is usually the smaller of the two lumens which is pulsatile in systole and seen as the inner contour on aortic arch views with evidence of systolic antegrade flow on colour Doppler with no evidence of thrombus or slow flow. Conversely, the false lumen is often larger with evidence of systolic compression and reduced systolic antegrade flow on colour Doppler. Thrombus can sometimes be identified in the false lumen. From a technical perspective, it is important that the view taken to acquire the images does not contain right heart structures above the aorta (eg standard PLAX view) as the contrast entering the right heart provides a ‘shadow’ on structures below preventing accurate image acquisition. In our experience therefore, the right parasternal and arch views are generally the most helpful. A key component of the image acquisition is the point at which the contrast influxes into the aorta and passes through into the false lumen. It is therefore important that a long loop is acquired at the time of first contrast administration. Image G The cases detailed above serve as a useful reminder that transthoracic echocardiography with trans-pulmonary contrast can be a useful ‘first line’ bedside investigation in patients with suspected Type A dissection when CT aortography or TOE are not immediately available. Laura Dobson, Stuart Moir Monashheart, Melbourne, Australia References 1. Nienaber CA, von Kodolitsch Y, Nicolas V et al. The diagnosis of thoracic aortic dissection by noninvasive imaging procedures. N Engl J Med. 1993; 328 (1): 1-9 2. Mulvagh SL, Rakowski H, Vannan MA et al. American Society of Echocardiography Consensus Statement on the Clinical Applications of Ultrasonic Contrast Agents in Echocardiography. J Am Soc Echocardiogr 2008; 21: 11791201 Image F PA G E 26 3. Evangelista A, Avegliano G, Aguilar R et al. Impact of contrast-enhanced echocardiography on the diagnostic algorithm of acute aortic dissection. Eur Heart J 2010; 31: 471-479 CONFERENCE REPORT BHVS Core Knowledge In Heart Valve Disease The inaugural Core Knowledge in Valvular Heart Disease (VHD) Study Day was held in Guy’s Hospital, London on Monday February 3rd. This educational initiative from the British Heart Valve Society (BHVS) is part of a range of educational activities designed to promote wider recognition and understanding of VHD. The key objective of this day was to deliver the BHVS syllabus on VHD, published recently by the BHVS and available online to all society members via the website. The concept of a Study Day was clearly appealing, as all 70 places were sold out by mid-January. Attending delegates comprised a mix of echosonographers, clinical scientists, cardiologists, GPs and cardiac nurse specialists. The structure of the Core Knowledge Study Day involved lectures delivered by UK experts in the field, commencing with Dr Jo D’Arcy (Oxford) who spoke on the changing epidemiology of VHD. The audience were reminded of the significant burden of VHD, increasing due to an ageing population. Importantly, she also alluded to changing patient expectations as many of our older population are fitter than in previous generations and thus more likely to expect intervention to restore their quality of life. Her talk was followed by excellent lectures from the current and past Presidents of BHVS, Professors Simon Ray (Manchester) and John Chambers (London) respectively, on aortic stenosis (AS) and aortic regurgitation (AR). Prof Ray highlighted several of thecurrent challenges in AS assessment, including low-flow low-gradient (LFLG) AS with depressed EF but also with preserved EF, also termed “paradoxical LFLG AS”. The pathophysiology of this condition was reviewed, as well as acknowledging that at present we have very limited data on the natural history of this condition and thus also the optimal management strategy. Prof Chambers discussed the causes of AR – including important causes of acute AR such as endocarditis, dissection and deceleration trauma – as well as reviewing the echocardiographic findings in acute and chronic AR and indications for surgery. It was highlighted that up to 20% aortic valves may be eligible for repair rather than replacement, although at present data on long-term outcome of repair versus replacement is scarce and there is limited surgical expertise with aortic repair in the UK also. Dr John Klein (London), consultant microbiologist, then gave a very thorough seminar on infective endocarditis (IE). The audience were reminded that incidence of Streptococcal endocarditis is falling whilst IE cases secondary to Staphylococcus species are on the rise. The critical importance of blood cultures – preferably before antibiotic administration (!) – was emphasised. Contemporary antibiotic protocols depending on organism were mentioned, as was a key South Korean randomised controlled trial (Kang et al New Engl J Med 2012) suggesting that early surgery is superior to “conventionally-timed surgery” for improving outcome (preventing embolic phenomena) in patients with large vegetations (>10mm length) with severe left-sided regurgitation.Dr Yassir Javaid, a GPwSI in Cardiology, then delivered an insightful talk on community aspects of VHD, detailing the assessments that can be made in primary care – including serial echocardiography – as well as sharing the model of valve clinic being developed between primary & secondary care in Northampton. It was incredible to see the power of the GP databases and how far behind we are in secondary care! In the final talk before lunch, Dr Phil McCarthy (London) spoke on mitral stenosis (MS). Although the least common left-heart valve lesion in Europe, it remains the dominant lesion in the developing world, in particular in sub-saharan Africa and the Indian sub-continent. After reviewing the pathophysiology of acute rheumatic fever, the key features of chronic rheumatic heart disease of the mitral valve – leaflet thickening, commissural fusion and chordal fibrosis / calcification – were discussed. Echocardiographic assessment of lesion severity and suitability for balloon valvuloplasty were also covered, with mention of the low number of highvolume operators for valvuloplasty in the UK. He finished with a fascinating and unique case in which a patient at King’s Hospital with a failing bioprosthetic mitral valve had undergone transvenous implantation of a TAVI device into the failing tissue MVR across an ASD – with an excellent result. The ASD was, of course, also closed on the way out! After lunch, Dr Anita MacNab (Manchester) gave a detailed overview of mitral regurgitation (MR), highlighting the differences between primary (organic) and secondary (functional) MR, in terms of aetiology, echocardiographic assessment, management and timing of surgery. The adverse prognostic impact of ischaemic MR was also discussed. Dr Cathy Head (London) then gave a presentation on right heart valve disease, concentrating on tricuspid regurgitation in adult patients as well as highlighting the prognostic importance of pulmonary regurgitation, especially in congenital heart disease patients. Mr Chris Blauth, a London-based cardiac surgeon, then gave an interesting presentation on prosthetic heart valves. It is always useful for non-surgeons to hear the thoughts of our surgical colleagues and thus a surgeon’s viewpoint on contemporary prosthetic valves was indeed very helpful. For example, the choice of prosthesis was discussed at length, with a strong reminder that contemporary bioprosthetic valves have an expected longevity considerably greater than the 10yr figure often quoted to patients, and thus most patients >60yrs age would be offered tissue valves. The reasons for choice of bioprosthesis (e.g. stented vs. stentless) were also briefly touched upon. Finally, Dr Saul Myerson (Oxford) gave an excellent closing talk on the role of multi-modality imaging in VHD. He emphasised that cardiac MRI and CT should be used to complement echocardiography when echo alone is inadequate (e.g. poor windows, sub-optimal alignment for Doppler interrogation etc).He demonstrated the utility of CMR for assessment in AS patients as well as research led by himself in Oxford demonstrating the accuracy of quantitative CMR for assessment of AR, showing that regurgitant fraction (<33% or >33%)accurately predicted onset of symptoms or (other reason for) referral for surgery. He also discussed the ability of CMR to assess the mitral valve and provide accurate measurements of MR regurgitant fraction, as well as accurate serial LV volumes and EF. In conclusion, the first BHVS Core Knowledge in Valve Disease study day was, we hope, a successful event and we thank the day’s delegates for their attendance and attention. Feedback forms will be closely analysed so that we may improve the event further and BHVS plans to run this event on a regular basis. The event attracts both RCP CPD points as well as BSE re-accreditation points. Please visit the BHVS website (www.bhvs.org.uk) for further details. Dr Benoy N Shah Imaging Fellow, Southampton PA G E 27 Echo in Africa 2014 By now we hope you have all heard about our humanitarian mission for 2014. A team of BSE volunteers will be travelling to Cape Town, South Africa to scan secondary school students for signs of Rheumatic Heart Disease. This will be the first in a series of humanitarian screening camps that we plan to run in collaboration with Tygerberg Hospital in Cape Town. A dedicated, permanent scanning facility will be built with approximately 12 scanning stations on the Tygerberg site. At the same time as performing the screening echo, volunteers will also be collecting data for research purposes. The Children Four schools in rural areas of Cape Town have signed up to take part in the screening project. These students are from low socioeconomic communities – up to 90% of them live in shacks in extreme poverty with little or no access to healthcare. We won’t be able to scan all the students on this first visit – our target is 2,000. All students identified with RHD will be taken under the care of staff at the Tygerberg Hospital and receive appropriate treatment and follow up. Our volunteers Following an electronic mailing in December 2013, many of you have already registered as potential volunteers; thank you! Unfortunately our current indemnity and insurance policies mean that we will only be able to accept volunteers who permanently reside in the UK and Ireland for this project, however we will be looking into broader policies that will allow overseas members to participate in future screening camps. All selected volunteers will be required to find funding to cover their own flights and we’re working with a UK based travel company who will be able to organise charity fares or flexible booking fares for all travelling to Cape Town. This is an excellent opportunity for our members to use their training and experience to make a positive contribution to communities in need. How can you help? There are logistical and operational costs that will need to be covered such as accommodation, ground transportation, travel insurance, medical malpractice insurance and legal fees to name a few. BSE is working hard to secure external funding to go towards covering these costs and reduce any further fundraising burden on the volunteers. Whether you are volunteering to take part in the humanitarian camp or not, you can still be part of its success with a charitable donation. Annual subscription fees are due to be collected in April and this would be an ideal time to make a small donation to help with this humanitarian project. PA G E 28 Direct Debit Members who pay their annual subscription by Direct Debit are invited to add a donation amount and complete and return the authorisation form below. We will be able to make a one-off collection from your account. Standing order/Cheque Members who pay by standing order or cheque can still complete and return the authorisation below to authorise gift aid but you will need to make a one off adjustment to your payment amount. Online donations If you make your payment online we are in the process of setting up an account with Virgin Money Giving which you will be able to donate via. Your support of this project is greatly appreciated. If you are a UK tax payer please remember to read and tick the box for gift aid as we will be able to claim back from the tax office an extra 25p in funding for each £1 you donate. Please do donate whatever you can. Your donation WILL help to save a life. If you need another gift aid form or know a non-member who would like to donate please visit the BSE Website www.bsecho.org. Please tick either of the first two boxes, remember to enter your donation amount. Please also tick the third box so that we can claim gift aid. My membership fee is currently collected by Direct Debit. In addition to my annual fee I wish to make a one off donation of £_____ towards the 2014 British Society of Echocardiography Echo in Africa project. I currently pay my membership fee by standing order or cheque. In addition to my annual fee I am donating £_____ towards the 2014 British Society of Echocardiography Echo in Africa project. Gift Aid: I confirm I have paid or will pay an amount of Income Tax and/or Capital Gains Tax for the current tax year (6 April to 5 April) that is at least equal to the amount of tax that all the charities and Community Amateur Sports Clubs (CASCs) that I donate to will reclaim on my gifts for the current tax year. I understand that other taxes such as VAT and Council Tax do not qualify. I understand BSE will reclaim 25p of tax on every £1 that I have given. Membership No. Forename House No/Name Date Surname Postcode Signature PA G E 29 LETTER TO THE EDITOR Introducing Echo Research and Practice – a new international journal, opening for submissions in March 2014. Over recent months, the British Society of Echocardiography has been working with Bioscientifica – an international biomedical publisher – to plan the launch of a major new journal for the echocardiography community. We’re delighted to announce that Echo Research and Practice will open for submissions by the end of March. Why is a new journal required? The field of echocardiography is rapidly expanding, and increasingly our work intersects with those in associated disciplines and beyond. Echocardiography has become a multimodality technique in its own right with subspecialisation in three-dimensional, transoesophageal, stress and interventional echocardiography. A lot of authors find it difficult to publish their research due to the very limited number of journals dedicated to echocardiography. Open access publication offers new ways to help communicate research discoveries more widely. The vision for our new journal is that it will draw from these two opportunities to create a powerful new platform through which we can accelerate research, education and practice in echocardiography for all disciplines that use the technique. Echo Research and Practice will be the first open access journal in echocardiography. All articles will be free to read to a global audience, with the journal funded by article publication charges (usually covered by the authors, their funder or institution). This unrestricted access offers exciting opportunities for our community to forge new connections, and find innovative ways to improve cardiovascular care. Publication in Echo Research and Practice will be free for all articles submitted for publication in 2014. As you are a member of the British Society for Echocardiography, I hope you will support this new initiative by submitting your best work, and becoming a regular reader. For more information on how to submit an article, and also to sign up to receive news on the first articles as they are published online, visit: www.EchoResPract.com. Professor Petros Nihoyannopoulos, Editor-in-Chief, Echo research and Practice Fold on this line and place in a DL window envelope BSE, Docklands Business Centre, 10-16 Tiller Road, London, E14 8PX PA G E 30 LIFETIME ACHIEVEMENT AWARD Gill Wharton At the last annual meeting in Liverpool I had the honour to present Gill with the BSE Lifetime achievement award. As well as being my mentor and manager for 20 years she is also a close personal friend of mine. As a student echocardiographer starting my career in 1980 she taught me everything I needed to know about echocardiography, congenital and acquired heart disease and professionalism. Gill has over 37 years experience as a sonographer, starting her career in 1976 at St Georges Hospital London working with Graham Leech. After this she worked briefly in Oslo as a research sonographer, before returning to the UK to work for Smith Kline, teaching cardiac departments the emerging technique of 2D and M mode. It was during this time that she met Gordon Williams who was so impressed with her that he went out of his way to secure her a job in his department. In 1980 she started work as a research echocardiographer at Killingbeck Hospital in Leeds. What makes Gill special as an echocardiographer is her passion for education and research. In the early 1980’s the field of echocardiography was a rapidly progressing field, developing from 2D and M mode to new modalities of PW then CW Doppler followed shortly by CFM. Echocardiography was no longer just for the tertiary centres; DGH’s wanted the same technology and their own departments. This meant clinicians and sonographers needed to be taught and for many years Killingbeck delivered its annual Doppler courses. Gill was an integral part of the faculty. Her reputation as an expert and teacher was recognised and she was invited to teach on the Salford BTEC echo course, which she did annually for over a decade. At the same time her job at Killingbeck continued to grow she worked closely with research registrars, teaching them echo and then assisting with their research projects. Her enthusiasm for research has never faltered over the years and her up to date CV includes over 40 publications and abstracts. In the early 1990’s she worked with the Leeds University to develop a Masters programme for medical ultrasound that was open to both radiographers and cardiac physiologists. Up to this time only radiographers had been able to access formal academic teaching at Masters Level. Gill wrote, taught and examined on the new programme. In 2005 Gill became the 1st consultant sonographer in the country. As an expert in congenital heart disease she developed a small team of highly specialist echocardiographers. She ran her own sonographer led fetal echo clinics for mothers with a family history of congenital heart diseases. As part of her role as a consultant she developed and implemented a training programme for screening of the fetal heart. She travelled to obstetric ultrasound departments across Yorkshire, Humberside and North Trent regions, where she trained the staff to image the fetal heart in multiple planes to significantly increase the dection rates of congenital heart disease in unborn children. Gill has been a part of BSE since the beginning; she has been an elected council member, a senior log book marker and a member of the Education committee. She has more recently joined the departmental accreditation committee. She was the lead author of the guidelines for chamber and valve quantification and a standard transthoracic study. Many of you will have these guidelines on your echo room walls and will be impressed with the beautiful images used in the posters. Gill provided all these and they are accurate examples of what she obtains on a day to day basis when scanning patients. She never cuts corners and always leads by example. She represents BSE at the DOH and has been involved with MSC, developing the curriculum for STP. She protects the profession and strongly defends the position that echocardiography should only be at scientist level. In 2008 as recognition of her work within the field of echocardiography she was awarded the rare honour of the fellowship of the American society of echocardiography. Many of you will have been influenced by Gill in your day to day work. Whether you have worked directly with her in Leeds, or have been taught by her on courses she has been involved with, or by use of the BSE guidelines I am sure Gill will have made a positive impact, and it is for this reason I nominated Gill for the BSE life time achievement award. Jane Allen, Vice President We now invite nominations for 2014 award. Can you think of someone you feel should be formerly recognised for their contribution to the field of Echocardiography? Let us know who, and why they should receive the lifetime achievement award. All submitted nominations will be considered by BSE Council. Nominations must be sent to [email protected] by 27th June 2014. PA G E 31 BSE Practical Competence Assessment Pilot Available for all logbook submissions Location: Wythenshawe Hospital, Manchester Date: Sunday 1st June 2014 Time: 9am – 5pm. Candidates will be allocated a 2hr time slot in their confirmation letter The BSE are modernising the current accreditation process and are looking for 50 candidates who would like to participate in our pilot scheme. This new practical assessment approach is designed to offer a more holistic approach to assessment. This pilot is aimed at candidates who are ready to submit their Logbooks and digital cases and are happy to attend a BSE accreditation examination day. Each candidate will be required to rotate through a 3 station system where formal review assessment of each element of accreditation would be completed. Station 1 Presentation of logbook portfolio, as per the current BSE Accreditation Requirements. These will be reviewed by a nominated BSE assessor. If successful, the candidate proceeds to station 2. If unsuccessful then the candidate is offered constructive feedback and would be welcomed to update their cases and submit through the current system. Station 2 Candidates perform a normal echocardiogram as directed by the BSE assessor. This will be preformed on a volunteer and not a patient. If successful, the candidate proceeds to station 3. If unsuccessful then the candidate is offered constructive feedback and would be welcomed to update their cases and submit through the current system. Station 3 1-on-1 viva examination, this will require candidates to provide 5 specific digital cases as per the current BSE Accreditation Requirements. A nominated BSE assessor will review a minimum of 1 of your 5 digital case submissions. The assessor will randomly select the case/s for presentation and there will be an opportunity to discuss the digital cases with the nominated BSE assessor. Success at this station will result in candidates passing all stations and they will achieve immediate accreditation. This will dramatically reduce the present time frame of 3 – 4 months. If this sounds like something that you would like to be a part of this process, please register your interest with Kemi in the BSE Accreditation Department by emailing [email protected] The success of this pilot practical assessment will result in an improved and updated BSE accreditation process. Please note, as this is a pilot to introduce a new process any individual who participates and is unsuccessful will not be penalised. This pilot will not be deemed as a first submission attempt and as such this will not effect your future submissions. So in essence this is a free attempt which may actually benefit the individual in the form of constructive feedback. Please note, this information could be subject to change. PA G E 32 BSE WORDSEARCH Circle the words listed below in the box at the bottom. WORDS TO SEARCH FOR ABCESS ABLATION AMYLOID ANEURYSM ANGIOGRAPHY ANOMOLY AORTA ASYSTOLE ARTIUM BICUSPID BIOPSY BRADYCARDIA CARDIAC CARDIOVERSION CAROTID CELLULAR CONSTRICTION DEGREE HAEMOCHROMATOSIS HYPERTENSION HYPOKINESIS MECHANISM MITRAL MYXOMA NASAL REGURGITATION RESTRICTION SARCOIDOSIS SINUS TACHYCARDIA TAMPONADE TUTORIAL VENTRICLE Many thanks again to Stuart Self for the latest puzzle. All correct entries will be put into a drawer to win £75 in vouchers. We are still waiting on a Winner for the Scrambled Echo (Issue 84), there is still time to re-submit PA G E 33 RECENTLY ACCREDITED MEMBERS Congratulations to the following members who have recently achieved BSE Accreditation Transthoracic Accreditation Racquel Alicmas, Heatherwood and Wexham Park NHS Trust Foundation Cheryl Allardyce, NHS Ayrshire & Arran Siobhan Armstrong, St George's Cardiac Investigations Dr Sajid Aslam, University Hospital of Wales Dr Graham Barker, John Radcliffe Hospital Dr Anthony J Barron, Harefield Hospital Mariam Chriszelle Batay, Queen Elizabeth Hospital Sonia Batty, Royal Berkshire Hospital Amanda L Beaumont, Calderdale and Huddersfield NHS Trust Michael Bird Sculeanu Bogdan, Newham Hospital Stephen Browitt, Leeds General Infirmary Dr Louise Brown, Southampton General Hospital Mitzi Bulquiren, St Mary's Hospital, Paddington Fiona Burchard, Royal United Hospital Bath Maria Burnett Howard Carter, Papworth Hospital Cecil Castillo, Northwick Park Hospital Victoria Cavanagh-Craig, County Durham and Darlington NHS Trust Joyce Krystel Cervantes, Basildon and Thurrock University Hospital Paul Charlton, Great Western Hospital Dr Simon Claridge, Poole General Hospital Margaret G Clarke, Great Western Hospital Lindsay Coates-Bradshaw Reuben Dane, Birmingham Heartlands Hospital Jihan Despuez, Oxford University Hospitals NHS Trust Nigel Dewey, Grantham & District Hospital Dr Vijay Dhakshinamurthy, University Hospital of Coventry Paul Edwards Claire Elliott, Morriston Hospital Richard Ewbank, James Cook University Hospital Naomi Farnon, University Hospitals South Manchester Eleanor Farrow, Norfolk and Norwich University Hospital Catherine Fernandez, Musgrove Park Hospital Cesar A Dos Santos Ferreira, Whipps Cross University Hospital Michelle Foster Nadia Francisco, Hampshire Hospitals Susan Geldard, Leeds General Infirmary John Gierula, Leeds General Infirmary Dr Mark Gilmore Dr Christopher Gingles, Ninewells Hospital Arioninson Pedro Gomes, Colchester General Hospital Marcos Gonsalves, Buckinghamshire Healthcare Charlotte Guanlao, Poole Hospital NHS Foundation Trust Lindsey Hague, Doncaster Royal Infermary Safia Hamid, Hammersmith Hospital Dr Andrew Hamilton, South West Acute Hospital Andrew Hancock, Northern General Hospital Dr Alan Harkness, Colchester Hospital Amanda Hayden, Worcester Royal Hospital Erica Jane Henry, Macclesfield District General Hospital Adam Hobbs, University Hospital Southampton Dr Hasan Iqbal Kim Isaac, Morriston Cardiac Centre PA G E 34 Allison Jones Carys Jones, Glangwili General Hospital Lesley Jones, Warrington and Halton Hospitals NHS Foundation Trust Rachel Jones, Diana Princess of Wales Hospital Faye Jowsey, Leeds General Infirmary Sarah Justice, Tunbridge Wells Hospital Satvinder Kahlon, Heart of England NHS Foundation Trust Dr Hazlyna Kamaruddin Dr Christina Kamperou, Russells Hall Hospital Steven Kane, Broomfield Cardiac Department Chelmsford Dr Afshin Khalatbari, Liverpool Heart and Chest Hospital Dr T W Koh, London Chest Hospital Dr Dipak Kotecha, University of Birmingham Daniel Lamb, Essex Cardiothoracic Centre Rebecca Leaning, New Cross Heart and Lung Centre Dr Joanna C Lim, Hammermsith Hospital David Lyth, Glan Clwyd Hospital Rebecca Macrae, The Heart Hospital Jayne Mahmoud, Lorn and Islands Hospital Marvin Manicad, Basildon and Thurrock Hospitals Julius Mas, Harefield Hospital Andre Mason, Russells Hall Hospital, The Dudley Group NHS Sheena Mathew, Addenbrook's NHS hospital Thomas McConnell, Royal Victoria Hospital Lukshmi McCormick, Northwick Park Hospital Jennifer McKinven, Glenfield Hospital, University Hospitals of Leicester Bruno Mendes, King's College Hospital Angela F Merrick, Norfolk & Norwich University Hospital Sarah Moon, Cardiff and Vale University Local Healthboard Emma Morgan, Addenbrooke's Hospital Lisa Morgan, Cavan General Hospital Asma Mullan, Queen Elizabeth Hospital, Birmingham Dr Tarique Al Musa Dr Govardhan Navaratnam, Nottingham City Hospital Fria Marie Nitura, West Middlesex University Hospital NHS Trust Reina Noblesala, Queen's Hospital Richard Nose, Basildon and Thurrock Hospital Dr Bartosz Olechowski, Royal Bournemouth Hospital Sevda Ozer, Royal Free NHS Trust Maria Paton, Leeds General Infirmary Sarah Ann Patterson, Morriston Hospital Gemma Priest, New Cross Hospital Nicole Purchase, Yeovil District Hospital Dr Shouaib Qayyum, The Royal Wolverhampton NHS Trust Dr Hindocha Rakhee, Royal Sussex County Hospital Dr Krishnaraj Sinhji Rathod, King George Hospital Dr Robin Ray, Royal Sussex County Hospital Simon Reece, Good Hope Hospital Emma Richardson, Portsmouth Hospitals NHS Trust Jonathan Ritchie, University Hospital of North Durham Laura Robinson, Sunderland Royal Hospital Elaine Rogers Jane Rogerson, Pinderfields Hospital Lisa Romanis, Royal Infirmary of Edinburgh Ian Rose, Gateshead Health Harpreet Kaur Sahemey, Hammersmith Hospital Dr Kulvinder Sandhu Dr Anshuman Sengupta, Bradford Royal Infirmary Emma Shannon, Manchester Royal Infirmary Ben Sinclair, East Sussex Hospitals NHS Trust Eswararaj Sivaraj, Southampton General Hospital Konstantinos Sivridis, Charing Cross Hospital Denise Skedd, New Victoria Hospital Rebecca Stanhope, Ninewells Hospital Christopher Stanton, The Royal Liverpool and Broadgreen University Hospitals Sally Stead, Salford Royal NHS Foundation Trust Louise Stevenson, Sheffield Teaching Hospital John Stewart, Sunderland Royal Hospital Nigel Stokes, University Hospital of North Staffs Dr Imran Sunderji, Castle Hill Hospital Garry Sykes, Leeds General Infirmary Dr Dewi Thomas, Royal Glamorgan Hospital Charlotte Turner, Leeds General Infirmary Dewet van der Westhuizen, Homerton Hospital Gail Vokes, Nottingham University Hospitals NHS Trust Eilish Walsh, Bon Secours Hospital, Cork Dr Malgorzata Wamil, Milton Keynes Hospital Dr Douglas Wan, Nottingham City Hospital Celina M Warren Natasha Watchorn, Mid Yorkshire Hospitals NHS Trust Alison Weedall, Countess of Chester Hospital Dr John Whitaker, University Hospital Lewisham Dr John Whitaker, St Thomas' Hospital Dr Aaron Wong, Morriston Hospital Dr Kee Fui Wong, NHS Tayside Dr Lisa Tze Mei Yung, Derriford Hospital DATES FOR YOUR DIARY 2014 BSE members can also see up-to-date details via the Events Calendar on the website www.bsecho.org 3rd & 4th April St George’s TOE Course Location: London Contact: [email protected] or www.toe-courses.com 4th April BSE Spring Written Exams Location: London, Belfast, Manchester, Bridgend & Edinburgh Contact: www.bsecho.org 5th April BSE/ICE Joint Meeting Location: Hilton, Templepatrick Contact: www.bsecho.org or 0207 345 5185 9th – 11th April Foundation Echocardiography Location: Contact: [email protected] or www.midlandsecho.com or fax 01782 801820 28th – 30th April Wythenshaw Introduction Of Echo Course Location: Manchester Contact: [email protected] or 0195 4200 018 12th – 15th May Ealing Hands On Course Location: London Contact: Shahla Kaleen or Claire Turner or [email protected] or [email protected] 13th May Manchester TOE Simulation Workshop Location: Manchester Contact: [email protected] Dr Juqian Zhang, Queen's Hospital Transoesophageal Accreditation Amor Mia Alvior, Queen Elizabeth Hospital, Birmingham Dr Douglas Atkinson, Manchester Royal Infirmary Dr Katrin Balkhausen, Oxford University Hospitals Dr Ahmed Bashir, Walsall Manor Hospital Dr Navtej Chahal, Royal Brompton Hospital Dr Laura Dobson, MonashHeart: Heart Specialists and Heart Care Delfin Encarnacion, Barts Health Trust Dr Christopher Hayes, Royal Bournemouth Hospital Dr Yasmin Ismail, University Hospitals Bristol Dr Afshin Khalatbari, Liverpool Heart and Chest Hospital Dr Dipack Kotecha, University of Birmingham Dr Jonathan Rosser, Sheffield Teaching Hospitals Departmental Accreditation Gold Standard Health LLP Nottingham University Hospitals NHS Trust. Russell Hall Hospital, Dudley University Hospital Southampton 21st – 22nd May Core Knowledge Location: Nottingham Contact: www.bsecho.org 21st – 23rd May Third Milton Keynes Advance Echocardiography Course Location: Milton Keynes Contact: [email protected] 24th June Manchester TOE Simulator Workshop 2014 Location: Manchester Contact: [email protected] 11th July Joint BSE & BHVS Meeting Location: Kings College, London Contact: www.bhvs.org.uk 16th – 18th July Foundation Echocardiography Location: Stoke on Trent Contact: [email protected] or www.midlandsecho.com or 0178 2801 820 16th September Manchester TOE Simulator Workshop Location: Manchester Contact: [email protected] 3rd – 4th October BSE Annual Clinical & Scientific Meeting & Exhibition Location: Birmingham Contact: www.bsecho.org Full details and course descriptions for all these courses are available from the BSE website. PA G E 35 CALL FOR ABSTRACTS 2014 We are pleased to announce that we are now accepting abstracts for the 2014 BSE Annual Meeting taking place in Birmingham. The template for submission is available from the BSE website www.bsecho.org.Both Technical and scientific submissions are welcomed. For 2014 abstracts will be given as poster presentations only in the Exhibition hall on Friday 3rd October. BSE members working in echocardiography who are participating in research are invited to submit Scientific or Technical Abstracts summarizing their project. We are particularly keen to receive submissions from echocardiographers or departments reflecting novel working practice, advances in echocardiographers or interesting audits. The following rules must be noted: • More than one submission may be entered from a department, as long as there is a distinct difference between each subject. • All submissions will be judged by a panel of experts. • The best submissions will be presented at the BSE Annual Conference on Friday 3rd October in Birmingham; the lead Author of the submitted abstract must be available to present on that date. The Lead Author will be asked to talk through their work live and then be available then to answer questions. • Lead authors of submissions accepted for presentation will have their registration fee for the day of presentation waived. Early bird fees will apply for Saturday 4th October if attending. • The lead author will present the abstract for approximately 5 minutes followed by 5 minutes of audience questions. • The presentation will be judged by an expert panel. • The winner will be invited to write a summary of their work for publication in ECHO, the journal of the BSE. Abstracts are summaries of work and may contain elements of work that have been/will be submitted to other international meetings (such as Euroecho) and other UK Meetings. • Based on the overall score (written abstract submission plus oral presentation), the British Society of Echocardiography investigator of the Year (2014) will be awarded. The solution to the shortage of echocardiographers? Both Mum, Clare Jackson and Dad Justin Adams are members of the BSE. This is their Son Samuel Adams, he picked up the Echo Magazine while having his nappy changed for a quick read. PA G E 36 LEAD CARDIAC PHYSIOLOGIST/DEPUTY CARDIOLOGY MANAGER We have a fantastic opportunity for a Lead Cardiac Physiologist/Deputy Cardiology Manager to join the fantastic, friendly team at The Lister Hospital, Chelsea. The post holder will provide specialist clinical knowledge and skills across a broad range of cardiac physiological investigations and deliver expert care for patients whilst supporting and developing more junior members of the team to ensure consistently outstanding levels of patient care. As the Cardiology Manager is predominantly based at another facility, the Lead Cardiac Physiologist will have the opportunity to lead the department in a fairly autonomous nature whilst also assisting with various management tasks, such as budgeting, auditing and developing the service provided. The right person for this role will have extensive Cardiology experience, with a BSc in Clinical Physiology (or equivalent) and be BSE accredited. They will also be extremely patient focused with a desire to drive a consistently high level of patient care, be flexible and adaptable and keen to share their skills and knowledge with the team. The Lister Hospital has an international reputation for providing high quality private healthcare to patients across a wide range of specialties. For medical professionals that value great training and career progression opportunities, an open-door management policy and a real team spirit, it’s the career destination of choice. To apply please visit our website www.hcacareers.co.uk You’re in goo d han ds C A REER S AT HCA HOSPITA L S Advanced Cardiac Physiologists in Echocardiography BSE Accredited Band 7+ Location: Oxfordshire (0.6 wte up to Full Time) £44,000 per annum pro rata plus car allowance, expenses and company pension. Sessional Staff Due to expansion in Community Services, we are also looking for staff to join our team in the following locations:Chertsey – Cobham – Leicester – Stoke Echotech is at the forefront in the drive towards community based echocardiology services in the UK. We are seeking suitably qualified Cardiac Physiologists to work as part of our expanding team providing imaging and reporting in community based NHS sites. Please apply in writing with a copy of your current CV to: Jenny Tonkinson-Hoare – Clinical Operations Manager [email protected] SAVE THE DATE! BSE Annual Meeting & Exhibition 2014 will be held @ The International Convention Centre, Birmingham on 3rd & 4th October. Registration will open soon. A full provisional programme will be placed on the BSE website www.bsecho.org Closing Date: 1st May 2014 PA G E 37 •••• NEW FOR 2014 •••• This year there will also be an option for hands on training using simulators. Delegates will be allocated in small groups to various centres across the UK within 3 months of the course (free of charge) for supervised training on a simulator. This will be useful for those in the early stages of echocardiography to improve their skills and for experienced operators to understand 3D anatomy using a computer model. Core knowledge in Echocardiography 2014 BSE points – Core Knowledge has now been awarded 6 points towards BSE re-accreditation (3 per day). •••• NEW FOR 2014 •••• Post Graduate Centre, Nottingham University Hospitals, City Campus Wednesday 21st and Thursday 22nd May 2014 Course fee £250 This is a 2 day course covering core topics in adult echocardiography. Course Cours ursee content conte ntent will be be delivered de by experts in the field of echocardiography and will cover the core knowledge wledge aand nd curre current rrent recommendations for assessment of various conditions. In addition to didactic lectures, lectures lectu res, there re will be interactive case discussions on various topics with tips and tricks for assessment. You will have the opportunity to test your knowledge and improve confidence using self marking theory and video questions. The course is aimed at anyone starting out in echocardiography or those wishing to refresh their knowledge. The course covers the majority of the syllabus for echocardiography accreditation examination and is ideal for those wishing to sit the BSE exam in the next 6-12 months. Topics covered Normal views and minimum data set Practical physics and image optimisation (how to make the best use of the ultrasound machine) Ischaemic heart disease and LV function – principals and methods of assessment; Right heart assessment including tricuspid and pulmonary valve Aortic valve disease Mitral valve disease Approach to adult congenital heart disease (CHD) Cardiomyopathies Echo in emergency medicine Prosthetic valves Reporting a transthoracic study Cardiac masses and endocarditis Hemodynamic assessment Course fee includes handouts, refreshments and lunch. Local accommodation details available on request. Feedback from September 2013 “Very useful and well run course. Good variety of topics covered - useful for refresher with measurements etc and very useful for things that are not commonly done in every case.” “Very in-depth course covering a vast array of topics. Thoroughly enjoyed all lectures and look forward to putting all I have learnt over the last 2 days into practice. Many thanks.” “Excellent course” To register please go to www.bsecho.org For further details including session extracts please go to www.bsecho.org/events-courses/core-knowledge/ BSE members will need to register online. PA G E 38 Non members will be able to print off a paper registration form. Advanced Imaging Day 7 9th May 2014 Royal Society of Medicine, London Advanced Imaging in Hypertrophic Cardiomyopathy Sessions will include anatomy, diagnosis, the roles of multimodality imaging and pitfalls. Presenters will include anatomists, surgeons and interventionists. The day is suitable to all involved in the care of patients with Hypertrophic Cardiomyopathy, since it offers a holistic approach to their care with a focus on imaging such hearts. 5 BSE reaccreditation points have been allocated to this meeting and CPD points have been applied for. For further details and to register please go to www.bsecho.org/events-courses/advanced-imaging-2014/ COMMUNICATING WITH THE SOCIETY Dawn Appleby [email protected] - 020 7345 5185 BSE, Docklands Business Centre, 10-16 Tiller Road, London, E14 8PX Tel: 020 7345 5185 Fax: 020 7345 5186 We can also be contact via email to: General and Post Accreditation (membership, re-accreditation, Distance Learning) Chris Grant at [email protected] Accreditation (exams, logbook submissions) – Kemi Olanrewaju at [email protected] Financial matters (payments, direct debits, duplicate receipts) – Ingrid Daniel at [email protected] Meetings and Events – Dawn Appleby at [email protected] [email protected] - 020 7345 5185 For submission of educational articles or case reports for ECHO: Dr. Gordon Williams at [email protected] and/or [email protected] PA G E 39 Irish Cardiac Echo & Imaging Group I.C.E. Joint BSE & ICE Meeting Saturday 5th April 2014 Hilton Templepatrick, Belfast This one day meeting will be held the day following the BSE spring accreditation exams taking place at the same location in Belfast. Provisional Programme (subject to amendment) • Surveillance of aortic regurgitation – just the LV? • Is low gradient low flow just moderate AS? • Defining ischaemic MR on echocardiography • A systematic approach to ACHD on TTE • Ventricular Septal Defects • Is TR enough in pulmonary hypertension? • Echo in CRT – dead as a dodo? • Stress and Perfusion – now required reading • Echo assessment of the RV – still a step too far? • DICE Cases: The Weird and the Wonderful The day has been approved for 5 BSE re-accreditation points. CPD points have been applied for To register to attend please go to www.bsecho.org/events-courses/bseice-meeting-2014/ The pre-registration fee is £65 per person. All registrations will be processed in GB£. Onsite accommodation is available. PA G E 40
© Copyright 2026 ExpyDoc