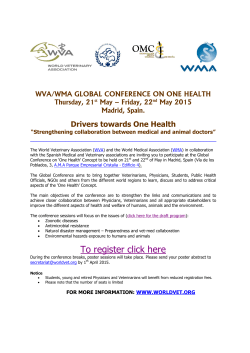
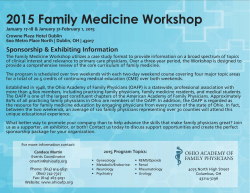
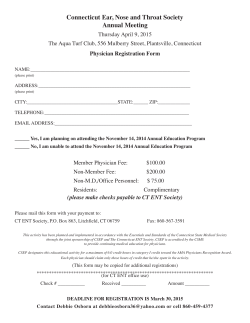
CLINICAL AND COMMUNITY STUDIES 0 ETUDES CLINIQUES ET COMMUNAUTAIRES Medical direction and control of emergency medical services in Canada James M. Thompson, MD, CCFP (EM); D. Gilchrist Curry, MD, FACEP, FRCPC Objective: To determine the level of physician involvement in prehospital emergency medical services (EMS) in Canada, as compared with published principles of medical control and direction. Design: Mail and telephone survey by means of a questionnaire from March to November 1991. Setting: All Canadian provinces and territories. Participants: Fifty-six key prehospital EMS physicians, senior government administrators and senior representatives of the agencies responsible for licensing physicians in each province or territory. Main outcome measures: Responses to questions regarding the legislation, organization, administration, practice and regulation of medical direction and control by physicians in each province or territory. Results: EMS legislation describing medical direction and control was completely lacking in five provinces and both territories and was incomplete in the remainder. Provincial guidelines written by physicians for prehospital patient care were present in only four provinces. Formal organization of medical directors varied from none to partially remunerated networks. Regional medical-director systems were present in three provinces, and local medical directors were required for all communities in three. Most rural ambulance services were found to engage physicians only when there was local interest. Conclusions: The level of physician involvement in the medical direction and control of EMS appears to be inconsistent across Canada and insufficient in most jurisdictions, as compared with accepted principles. Objectif: Determiner le niveau de participation des medecins aux services medicaux d'urgence (SMU) prehospitaliers au Canada par comparaison avec les principes publies sur la direction et le contr6le medicaux. Conception: Sondage postal et telephonique au moyen d'un questionnaire de mars A novembre 1991. Contexte: Toutes les provinces et les territoires canadiens. Participants: Cinquante-six medecins cles prodiguant des SMU prehospitaliers, cadres superieures du gouvernement et representants principaux des ordres des medecins de chaque province et territoire. Principales mesures des resultats: Reponses aux questions sur les lois, l'organisation, l'administration, l'exercice et la reglementation de la direction et du contr6le medicaux par les medecins dans chaque province ou territoire. Resultats: Les lois sur les SMU decrivant la direction et le contr6le medicaux faisaient Dr. Thompson is a rural physician in Sundre, Alta., an assistant clinical professor in the Faculty of Medicine, University of Calgary, Calgary, Alta., and past president and secretary-treasurer ofthe Alberta Association ofEmergency Medical Services Physicians (AAEMSP). Dr. Curry is a clinical lecturer in the Faculty ofMedicine, University of Calgary, founding president ofthe AAEMSP, chairman ofthe Urban Medical Control Committee, AAEMSP, former medical director, City ofCalgary Emergency Medical Services, and a former member of the CMA Conjoint Committee for the Accreditation ofEducational Programs in Emergency Medical Technology. Reprint requests to: Dr. James M. Thompson, PO Box 930, Sundre, AB TOM IXO - For prescribing information see page 2048 CAN MED ASSOC J 1993; 148 (1 1) 1945 completement defaut dans cinq provinces et les deux territoires, et elles etaient incompletes dans les autres provinces. Des lignes directrices provinciales redigees par des medecins sur les soins prehospitaliers aux patients n'etaient presentes que dans quatre provinces. L'organisation officielle des directeurs medicaux variait de nulle a des reseaux partiellement remuneres. Des reseaux regionaux de directeurs medicaux etaient presents dans trois provinces, et trois d'entre elles exigent des directeurs medicaux locaux pour toutes les collectivites. La plupart des services ambulanciers ruraux, a-t-on constate, n'engagent des medecins que lorsqu'un interet local se manifeste a cet egard. Conclusions: Le niveau de participation des medecins a la direction et au contr6le medicaux des SMU semble variable a travers le Canada et insuffilsant dans la plupart des provinces et des territoires par comparaison avec les principes reconnus. F ew areas of medicine in Canada are experiencing a more explosive evolution at present than prehospital emergency medicine. The process involves extraordinary technologic and legislative changes. Because of the many interest groups involved it has created a unique kind of social turmoil as these groups attempt to define their roles. Physicians with a special interest in emergency medical services (EMS) are concerned that the best interests of patient care be served during this evolutionary period. In a landmark 1986 paper Holroyd, Knopp and Kallsen' provided a fundamental definition of medical control of prehospital care: a "system of physician-directed quality assurance that provides professional and public accountability for medical care in the prehospital setting." The Alberta Association of Emergency Medical Level EMT-1 EMT-lI Services Physicians (AAEMSP) has been committed to this definition,2 because it views prehospital care as physician-directed care practised outside the hospital in a unique and difficult environment. Pre- hospital patients cover the entire spectrum with regard to age and the type and acuity of clinical problems; these patients can be some of the sickest and most desperate in the health care system. Although prehospital-care providers are recognized experts in the safe extrication, transport and initial treatment of patients, the level of medical training and experience of even the best-trained emergency medical technician is considerably less than that of a physician (Table 1). The definitions and principles accepted by the AAEMSP for the terms "medical direction," "medical control" and "medical advice" are shown in Table 2. The principles of these new physician roles Description of accredited program 180 to 260 h of instruction, 24 to 72 h of hosppil experience, 25 to 30 calls of.r*otlcum Basic lfe su wtils: s l patient ass mt, erication and sinp tipt m. including ba-valve-mas ventilation 200 to 208 h of iruction, 36 to 92 h of hospital experience, 20 to 60 h of am a practicum EMTi- soope of prctice, with some advancd lb urt ills (e.g., Provinces with accredited program British Columbia Alberta Saskathwan MeMba -Prince Edwuard sland Newfoundiand British Columbia Manitoba * _t $ F wlf:oytng mitkvy t1tlhekIoser, admin roig ni xide and EMT-I1I 1Qto3Swkpfi su ion, 7to British Columbia Albet andrdtr mdns by various routles 1946 CAN MED ASSOC J 1993; 148 ( 1) 19 LE ler JUIN 1993 have evolved over the past two decades.6-'0 Although nonphysicians can and should be involved in medical control, it has been argued by EMS physicians and others that physicians must be involved intimately and authoritatively for medical control to be effective.6-22 The medical direction and control of EMS by Canadian physicians has been encouraged in position papers by the Canadian Association of Emergency Physicians,23 the AAEMSP2,24 and the Department of National Health and Welfare." The medical direction of educational programs in emergency medical technology is -mandatory according to the guidelines for accreditation issued by the CMA,3 and it is encouraged widely.'2 The AAEMSP believes that an EMS system in which physicians provide medical direction to ambulance services and medical control of all levels of prehospital care should be present in every Canadian community. Despite these calls for physician involvement we suspected that problems exist in the organization of medical direction and control across Canada. We conducted a survey to determine the current level of physician involvement in EMS relative to the principles outlined. identified as senior EMS consultants to the government in their province or territory or if they were known to be active leaders in EMS development. We did not attempt to trace all active EMS physicians, assuming that a few key representatives could describe the situation adequately. Each participant was asked a series of questions: Does existing legislation mention medical direction and control? How are medical direction and control practised in urban and rural areas? Do ambulance services engage physicians to act as medical directors? Is there an organization of medical directors? Are there provincial protocols for prehospital patient care and are physicians involved in their development? Does the provincial government engage physicians to sit on an advisory committee or act as provincial medical directors? Does the agency responsible for licensing physicians play a role in EMS? We interviewed the 56 participants by telephone if the written response was incomplete or missing, achieving a response rate of 100%. The answers to the questions were compared with the ideal definitions already described. Methods From March to November 1991 we wrote and telephoned 56 key physicians, senior administrators of the government agencies responsible for ambulance services and senior representatives of the agencies responsible for licensing physicians in each province and territory. Physicians were chosen if they were formally Results The organization of medical direction and control varied tremendously across Canada, from a highly organized system in British Columbia (where a network of partially remunerated regional and local medical directors is fostered by the provincial government) to virtually no formal medical control in some regions (Table 3). Ambulance services in most small communities in Canada were not expected to engage local physicians to act as medical directors, except in British Columbia, Alberta and Degree of Term Medical diretiion r; Medical contr( D1 Prospective -* Immediate patient care in person.or by voice Retrospecti yve Chart review, quality assurance, risk *Adap~sd authority Variable Considerable design Direct Medical advice JUNE 1, 1993 Definition* -Advice or directives given oto an ambu4ance or dispatch service ..Orders given to ambulance attendants: Protocols, standing orders, training and system -tlecommunication management Advice- given to an organization other than an armibulance or dispatch service Little rom Rein.6 CAN MED ASSOC J 1993; 148 (1 1) 1947 directors except in Alberta, where prospective and retrospective medical control is required. (By sufficient we mean that the legislation specifically requires at least some of the three types of medical control defined in Table 2.) Direct medical control was well developed in many but not all major urban communities. It was found that basic life support services throughout Manitoba. Systems of regional medical direction found in Saskatchewan and Ontario. EMS legislation was not present in five jurisdictions, although it is planned in four of these (Table 4). In the remaining seven, medical control was reportedly legislated in only two provinces, and medical directors were required in only four. None of the legislation gave sufficient authority to medical were ... Z ..., .SW.' *NO Til .. .. .. m. tZ. Ys ... ,2s;,L,&,&, s.v_ SS ..i Yes. ~yes yes. . . .~ ~ ~~~O No Yes yes No:* .: NO' ., in M. ry WWM; NO u.' Yes n *vesi fhI No NO' N nd No ILA .dm 1-L'f1 _A `... -'- -...i -7 * 1948 . CAN MED ASSOC J 1993; 148 ( 1) 19 LE 1 er JUIN 1993 Canada tend to operate without direct medical control, so that physician-directed care usually does not begin until the patient reaches the hospital. Prospective medical control was present to some extent in all the provinces. Protocols are developed by physicians at a provincial level in only three provinces (Table 3). In others protocols are developed locally for some advanced life support skills. In several provinces physician involvement in protocol Provinc or territory British Columbia Alberta Saskatchewan Manitoba Ontario QQuebec New Brunswick development has been very limited. Retrospective medical control was required in a few jurisdictions but was not universally applied or enforced in any province. The CMA recommended that the agencies responsible for licensing physicians be responsible for identifying medical acts that may be delegated to ambulance attendants.4 These agencies were found to have variable and often limited involvement with Medical diretcion *or control features. AlIows. attendant to perform emergency procedures until a vihyecian is available. Establishes.guidelines for local medical diectors, termed "local. medical coordinators." Health Disciplines -Ac Defines prospective and retrospective medical control and EMT scopes of pract!e.i9. EMT can praotis only. while uidet'medical control. Proposed amendment adds direct mediCal control. Ambulance Servicas Act Might require that each ground ambulance service engage a medical . (pending) director and each ground ambulance -boarden a medical adviser. Defines prospective and direct Ambulance Act medical oontrol. Ambulance Servicas.Act Specifies that each ambulance service must name a medical adviser or medcal director. Ambulance At (piIanned, - Allo.ws physicians to determine the * receiving hospital. Defines base hospitals and base-hospital . physicansbut.only.defines relationship to ambulance attenda.nts in general terms. *Health S.ervices AI,cit Medical control legislation planned. The Qorporation d'urgences-santb de Ia.r6gion de Montrhal M6tropolitain s. required to appoint a .member from the emergency department * coordinators of Montreal hospitals.25 Ambulance Servicaes Act No reference to medical direction or. control. Proposewd leislaton states that an attendant will not EMS legislation Health Eme. rgen4y Actu Nova Scotia Prince Edward Island Planned Public Health Act Newfoundland Motor Carrier Act Northwest Territories Yukon Territory None practise outside scope of ractice (basic life support) without deiegation from a-physician. Major changes to the existing legislation are planned. Requires services using defibrillation to have a medical adviser. Under the planned "EMS act" the government proposes to require a medical director for each service. No reference.to medical direction or. control. JUjNE 1, 1993 Planned. CAN MED ASSOC J 1993; 148 (1 1) 1949 v. , r R control of a physician, most services tend to identify~~~~~ EMS (Table 5). They tended to approve, in prin- control of a physician, most services tend to identify ciple, the delegation of specific medical acts to a "medical director"; this role is poorly defined. ambulance attendants but were not involved in developing protocols for use of these skills in pre- Saskatchewan hospital care. The provincial government has a policy stating that each advanced life support service must have a British Columbia medical director who doubles as a regional medical Ambulance services are owned and operated by adviser. The regional advisers form a committee the province, and medical control is exerted at all chaired by a provincial medical director, who is levels by a network of physicians. The senior phys- appointed by the provincial government. Protocol ician gives advice at meetings of the government's changes are submitted through the Saskatchewan multidisciplinary Pre-hospital Care Committee and Medical Association and the College of Physicians is a voting member of that committee. Recommen- and Surgeons of Saskatchewan for approval by the dations for changes to protocols flow up from local general medical community. There is no requiremedical directors through regional directors, and ment for basic life support services to have a medical changes are made at a provincial level. director. Alberta Manitoba A regulation of the Ambulance Services Act Planned regulations of new legislation (Ambulance Services Act) are expected to define the role of specifies that each ambulance service must have a physicians in EMS. Since registered emergency med- "physician adviser." This regulation is not enforced ical technicians must practise under the medical strictly because of the difficulty in recruiting phys- Province or territory Britsh Columbia Alberta Invodvement None 'Er o),W.kilnameonlyAH thdtegIohof "medical acts Nn&ifunswick' N*b pS protocols. Apov of a medical act but then is not ApprovEs irvolted with prtcol ddeveomnt. Appro.s. of awdlmcaat but then is not Has pubUshed i iWmR nW i protocol de Hped. gu5_Wines regarding the delbgation of medical acts and s regarding ptehospita care programs. Wilt ne involved wit issu resated to delegation of a medicalact when attendiants begin to funcon at a klevl hOgr than that of first aid. None Plans to se up a committee to ou d ted medical Prince Edward None Saskatchewan' ManitOa' Ontario* Quebect acts. a 9|t'SD stlpe iJju' Dpar o CM. 1950 CAN MED ASSOC J 1993; 148 (1 1) of _osn oiis 'd~ ~ ~ ~Ite a c an l"rb Aff*. . LE 1 er JUIN 1993 icians in rural areas. The provincial government tion and control are not required. There is a tentastrongly encourages physician involvement with tive plan to organize EMS into regions around EMS. The Provincial Medical Advisory Committee central hospitals. Local physicians hope to see medapproves protocols for use by local ambulance ser- ical directors required for these regional centres. vices. Prince Edward Island Ontario Each of the 19 designated base hospitals and 5 associate base hospitals in the province engages a physician to act as a medical director for EMS in the region served by the hospital. These physicians sit on a multidisciplinary committee called the Base Hospital Advisory Group, which reports to the provincial government. Base-hospital physicians influence ambulance services within their catchment area. Ministry of Health policy states that base hospitals "provide leadership and medical direction in the provision of prehospital and interhospital emergency health services within a specified geographic area in order to ensure that services provided are medically sound and well coordinated." The government's 5-year goal is to provide medical control to all ambulance services. Quebec Local physicians have been instrumental in assisting a community college to become accredited to train ambulance attendants. A few services have developed informal relationships with local physician advisers. The government has organized a multidisciplinary committee to recommend features of a planned "EMS act." Newfoundland The provincial government retains a part-time physician consultant for EMS issues. There are no specific plans for medical direction or control in planned EMS legislation. The request from interested physicians to delegate the medical acts of intravenous access and semiautomatic defibrillation to ambulance attendants was recently approved for one service after years of lobbying. Northwest Territories Although medical direction and control by physIn the western Northwest Territories a multidisicians has not been well developed in Quebec in the committee is attempting to set minimum ciplinary past, there is a strong movement by the provincial for EMS operations, but it has little standards government and concerned physicians to change The committee has produced limsupport. financial this. There are plans to develop provincial protocols written by physicians and to introduce new legis- ited prehospital-care guidelines. The region tends to lation that will encourage medical control and direc- rely heavily on charter aircraft for EMS transportation organized by St. John Ambulance and crewed tion at all levels of EMS. by trained nurses. A physician assists St. John Ambulance in organizing this service. New Brunswick In the eastern region nurses at the hospital in A multidisciplinary committee sponsored by the Iqaluit are trained for air ambulance escort, and provincial government is investigating alternatives under protocols evaluated by the medical staff at the for EMS regulation. The committee includes at least hospital they serve a wide area. Emergency medical one physician. Physicians are formally involved with technicians in the Iqaluit ground ambulance service EMS systems in larger, urban communities. A few work under direct medical control and are trained in small, rural services work with physicians informally part by local physicians. Neither the air nor the to develop protocols. Direct medical control is avail- ground ambulance system has a formal medical able in a few regional hospitals, which are linked in director. networks with primary care hospitals. Yukon Territory Nova Scotia Physicians are involved in writing EMS protocols for very few services. A multidisciplinary committee organized in 1990 by the Department of Health has completed a report recommending extensive changes. The department has agreements with individual ambulance services, in which minimum standards for the service are listed. Medical direcJUNE 1, 1993 Owing to the heavy reliance on air ambulance services, the government seeks advice from specialists such as obstetricians and pediatricians outside the Yukon Territory regarding some aspects of patient management; it also looks to the BC ambulance service for many suggestions. The government is contemplating major changes in the EMS legislation and plans to involve local physicians more CAN MED ASSOC J 1993; 148 (1 1) 1951 not necessary. We have found that considerable skill, knowledge and commitment is required to negotiate the grey areas between administrative functions and medical direction that can lead to conflict.26 Experienced EMS physicians clearly feel that Discussion medical direction and control can substantially imWe found that the legislation as well as the prove patient care;116-'9'22 however, published reorganization and practice of medical direction and search into this issue is scarce, and more should be control of EMS are at an early stage of development undertaken. in Canada. The ideal situation would be one in Until there is substantial evidence to the conwhich physicians participate in all three forms of trary, we believe that to achieve optimum medical medical control and provide medical direction to care for prehospital patients physicians must retain both regional governments and individual services the ultimate authority for patient care. As EMS in all communities. Given the strong calls for med- systems develop across the country politicians, hosical direction and control of EMS by physicians pitals, fire departments, owners of ambulance comwith experience in prehospital emergency medical panies, unions of prehospital care providers and care,6-101316-822 this finding suggests that a con- professional associations are all struggling for control certed effort to improve physician involvement of prehospital care. Knowledgeable, committed EMS is required. physicians are needed to provide leadership in this In many jurisdictions prehospital-care providers rapidly evolving area of medicine and to ensure the are evolving toward independent practice. They may appropriate use of increasingly complex and expenhave limited contact with other health care providers sive technology. Provincial legislation should be and can develop more allegiance to public service developed to formalize the need for appropriate agencies, such as the police and fire services. The physicians to have a major role in the design, AAEMSP believes that collaboration between emer- delivery and ongoing evaluation of all medical asgency medical technicians and knowledgeable, com- pects of EMS, including ambulance services, dismitted physicians providing medical control is essen- patch services and educational programs. tial for the provision of high-quality care based on sound, current scientific knowledge. Our belief, and We thank the government agents and the representatives that of others,62022 is that abdication of or exclusion of the physician-licensing institutions in each province and from this role increases the risk of inappropriate, territory who assisted us. We also thank the following for descriptions of medical direction and concost-ineffective and potentially dangerous prehospi- physicians in trol their regions: Drs. Charles Sun (British Columbia); tal medical care. Robert Johnston, Maurie Simpson, Ivars Argals, Chris Our study raises many questions for further Westover, Daryl Stewart, David Shragge, Terry Sosnowski, research. Our choice of survey questions and method James Davidson, Dennis Nesdoly, Peter Lindsay, Keith of identifying survey participants could have caused Spackman and Peter Gant (Alberta); James Cross and us to overlook some important findings. By exclud- James O'Carroll (Saskatchewan); Urbain Ip and Neil ing emergency medical technicians and EMS manag- Donen (Manitoba); Marion Lyver and Christopher Rubes ers we could not document their opinions or their (Ontario); Pierre Frechette, Marcel Boucher and Ted experience with physicians acting as medical direc- Leibovici (Quebec); Bertrand Laporte, Jane Findlater and tors. Since our survey did not include many phys- Robert Beveridge (New Brunswick); Edward Cain (Nova icians working in rural EMS systems or physician Scotia); David MacKenzie and Arthur Losier (Prince Edward Island); Vinod Patel (Newfoundland); Robert educators we might have missed some key phys- Williams and Paul Stubbing (Northwest Territories); and icians or administrators with special knowledge. Bruce Beaton (Yukon Territory). Finally, EMS systems are evolving in Canada so This study was funded by the Alberta Association of rapidly that our information for some jurisdictions Emergency Medical Services Physicians and the Governcould soon be out of date. ment of Alberta. It is not clear from our study why medical direction and control are not developed to the ideal References level we defined. Although we did not specifically ask about obstacles to physicians delivering medical 1. Holroyd BR, Knopp R, Kallsen G: Medical control: direction and control we heard about many, includquality assurance in prehospital care. JAMA 1986; 256: 1027-1031 ing inadequate physician training, psychologic resistance by emergency medical technicians who are 2. Alberta Association of Emergency Medical Services Physicians: Medical Control of Emergency Medical Services (posiattempting to establish their role, poor remuneration tion paper), AAEMSP, Edmonton, 1987 for physicians providing these services and a percep- 3. Conjoint Committees for the Accreditation of Educational Programs in Allied Medical Disciplines: Section H: Emergention by administrators that physician involvement is formally. One physician currently acts as a liaison between the territorial government and the Yukon Medical Association on EMS matters. 1952 CAN MED ASSOCJ 1993; 148 (11) LE lerJUIN 1993 cy medical technology (levels I, II, and III). In Basis of Accreditation for Educational Programs in Allied Medical Disciplines, Part II: Specific Accreditation Requirements and Guidelines for Educational Programs in Individual Allied Medical Disciplines, Can Med Assoc, Ottawa, June 1991: H 1H5 4. Conjoint Committee for the Accreditation of Educational Programs in Emergency Medical Technology: Competency Requirements for Graduates of Educational Programs in Emergency Medical Technology (Levels I, II and III), rev, Can Med Assoc, Ottawa, 1992 5. Conjoint Committees for the Accreditation of Educational Programs: Official List of Accredited Programs, Can Med Assoc, Ottawa, Jan 1993 6. Reines D: The emergence of medical control. In Kuehl A (ed): National Association of EMS Physicians: EMS Medical Directors' Handbook, Mosby, Toronto, 1989: 155-162 7. Krentz MJ: Off-line medical control. In Roush W (ed): Principles of EMS Systems, a Comprehensive Text for Physicians, American College of Emergency Physicians, Dallas, Conferences continued from page 1933 Aug. 31-Sept. 3, 1993: 5th International Congress on Ethics in Medicine London, England Castle House Conferences, 28-30 Church Rd., Tunbridge Wells, Kent, England TNl lJP; tel 011-44-892539606, fax 011-44-892-517005 a 1989: 95-100 8. Stewart RD: On-line medical control. Ibid: 101-108 9. McSwain NE: Indirect medical control. In Kuehl A (ed): National Association of EMS Physicians: EMS Medical Directors' Handbook, Mosby, Toronto, 1989: 163-174 10. Braun 0, Callaham ML: Direct medical control. Ibid: 175212 11. Health Services Directorate, Health Services and Promotion Branch: Guidelines for Establishing Standards for Special Services: Pre-Hospital Emergency Care Services, Dept of National Health and Welfare, Ottawa, 1985: 4-5 12. Hauswald M: Medical direction of the EMT training program. In Roush W (ed): Principles of EMS Systems, a Comprehensive Text for Physicians, American College of Emergency Physicians, Dallas, 1989: 175-180 13. McSwain NE: Medical control of prehospital care [E]. J Trauma 1984: 24: 172 14. Ryan J: Quality assurance in emergency medical services systems. In Kuehl A (ed): National Association of EMS Physicians EMS Medical Directors' Handbook, Mosby, Toronto, 1989: 213-232 15. Roush WR (ed): Foreword. In Principles of EMS Systems, a Comprehensive Text for Physicians, American College of Emergency Physicians, Dallas, 1989: 1-2 16. Boyd DR, Micik SH, Lambrew CT et al: Medical control and accountability of emergency medical services (EMS) systems. Trans Veh Technol [US Govt] 1979; VT28 (4): 249-262 17. Pepe PE, Stewart RD: Role of the physician in the prehospital setting. Ann Emerg Med 1986; 15: 1480-1483 18. Pointer JE: The emergency physician and medical control in advanced life support. J Emerg Med 1985; 3: 31-35 19. Krentz MJ, Wainscott MP: Medical accountability. Emerg Med Clin North Am 1990; 8: 17-32 20. Shanaberger CJ: Determining domain: the issue of medical control. J Emerg Med Serv 1991; July: 107-108 21. Stout J: Organizing quality control in EMS. J Emerg Med Serv 1988; Mar: 67-74 22. Pepe PE, Stewart RD, Copass MK: Prehospital management of trauma: a tale of three cities. Ann Emerg Med 1986; 15: 1484-1490 23. Canadian Association of Emergency Physicians: Medical Control of Prehospital Emergency Services (position paper), CAEP, Ottawa, 1986 24. Alberta Association of Emergency Medical Services Physicians: Provincial Medical Director of EMS for the Province of Alberta (position paper), AAEMSP, Edmonton, 1990 25. An Act Respecting Health Services and Social Services, RSQ (1989), c S-5, s 56-2 26. Tryon J: Medical control and direction. J Emerg Med Serv 1988; Dec: 67-70 JUNE 1, 1993 Sept. 5-9, 1993: European Atherosclerosis Society 62nd Congress Jerusalem, Israel Gil-Kenes, 946-1617 J.F.K. Blvd., Philadelphia, PA 19103, tel (800) 223-3855, fax (215) 568-0696; or Secretariat, 62nd European Atherosclerosis Society Congress, PO Box 50006, Tel Aviv 61500, Israel, tel 011-972-3-517-4571, fax 011-972-3-660-325 Sept. 9-11, 1993: 2nd International Congress on Peer Review in Biomedical Publication (sponsored by the American Medical Association) Chicago Annette Flanagin, North American coordinator, Peer Review Congress, JAMA, 515 N State St., Chicago, IL 60610, tel (312) 464-2432, fax (312) 464-5824; or Jane Smith, European coordinator, Peer Review Congress, BMJ, BMA House, Tavistock Square, London WC1H 9JR, England, tel 011-44-1-71-387-4499, fax 011-44-1-71-383-6418 Du 9 au 13 sept. 1993: Les soins specialises en crise? 62e Assemblee annuelle du College royal des medecins et chirurgiens du Canada Vancouver Anna Lee Chabot, chef, section des reunions et assemblees, Bureau des affaires des Associes, Colltge royal des medecins et chirurgiens du Canada, 774, prom. Echo, Ottawa, ON KIS 5N8; tel (613) 730-6233 ou (613) 730-8177; fax (613)730-8830 Sept. 9-13, 1993: Specialty Care in Crisis? - 62nd Annual Meeting of the Royal College of Physicians and Surgeons of Canada Vancouver Anna Lee Chabot, chef, section des reunions et assemblees, Bureau des affaires des Associes, College royal des medecins et chirurgiens du Canada, 774, prom. Echo, Ottawa, ON KIS 5N8; tel (613) 730-6233 ou (613) 730-8177; fax (613)730-8830 Oct. 10-15, 1993: 4th International Conference on Noninvasive Cardiology Limassol, Cyprus Ambassador Chevy Chase Travel, 2 Wisconsin Circle, Chevy Chase, MD 20815, tel (800) 424-8282, fax (301) 907-4787; or Secretariat, 4th International Conference on Noninvasive Cardiology, PO Box 50006, Tel Aviv 61500, Israel, tel 011-972-3-517-4571, fax 011-972-3-660-325 continued on page 1966 CAN MED ASSOC J 1993; 148 (1 1) 1953
© Copyright 2026 ExpyDoc