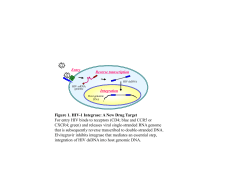
A BIT IF EVERYTHING! A GENERAL UPDATE Dr Laura Waters Consultant IMPORTANT DISCLAIMER This presentation contains medical and pharmaceutical news, and data, supplied for general information purposes only. The materials contained within this presentation do not constitute medical or pharmaceutical advice, which should only be sought from your own medical and pharmaceutical advisers. We are not responsible for any mistakes or deficiencies. The material displayed within this presentation is provided without any guarantees, conditions or warranties as to its accuracy. If you need medical advice or are planning to change anything relating to your healthcare or treatment please speak to your nurse or doctor before. A bit if everything! Laura Waters Consultant Content • • • • • • • • • Medical developments New treatments “Each speaker Trials gets max 15 mins Clinic response to the present situation - in order to keep it New services snappy” Partner study Proud study A slide on Hep C Do you want to mention Telemedicine? Medical developments (General Medicine) • NICE guidelines for primary prevention of cardiovascular disease – Change in threshold for when to give a statin – Controversial! • Nicotine patches + other drugs are more effective than either alone for smoking cessation New HIV treatments • Dolutegravir (Tivicay) – – – – Integrase inhibitor Licensed January 2014 Not (quite) available yet…. Draft NHSE guidance will probably be introduced with no/minimal changes…. June 2014 Clinical Commissioning Policy: Dolutegravir for treatment of HIV-1 in adults and adolescents Month 2014 Reference: NHS ENGLAND B06/P/b Some issues? • “Approximately 10% of HIV positive people cannot use the standard first line treatment (efavirenz) because of these side effects and approximately another 10% change treatment because of them up to two years after starting” 7. Criteria for commissioning Dolutegravir will be routinely commissioned in HIV-1 infected adults and adolescents in the following clinical scenarios: Patients unable to tolerate first line therapy Patients who are not suitable for or who do not tolerate efavirenz based first line therapy as agreed in the MDT (expected to be no more than 20% in the first two years of treatment). Dolutegravir is a treatment option for this patient group. Where used, this policy recommends use of dolutegravir with the lowest cost, clinically indicated backbone. This is generally abacavir and lamivudine. Patients failing treatment treatment and those with resistance Dolutegravir is approved for use in these patients requiring an integrase inhibitor due to recorded treatment failure or resistance: In treatment experienced and Integrase inhibitor naïve patients at a dose of 50mg daily. In treatment experienced and integrase resistant patients at a dose of 50mg twice daily. Dolutegravir should be combined with at least two other anti-viral drugs to which the virus is sensitive. All patients for whom dolutegravir is considered a treatment option for failure and resistance must be considered in an HIV specialist treatment multidisciplinary Exclusions • Patients switching to dolutegravir not referred to and discussed in the MDT meeting or where decision not recorded • Patients stable on treatment should not be switched, no published trial data • Use of dolutegravir by providers not commissioned by NHSE to provide HIV care and treatment services. • An increase in price would require a review of this policy. • Where clinicians consider switching outside these circumstances, an Individual Funding Request may be considered What this means for YOU! • Switches may be delayed while appropriate decisions made • The new drugs are probably not going to be used first-line unless good reason Other ‘new’ drugs • Cobicistat (Tybost) – – – – – Alternative to ritonavir ‘Built-in’ booster in Stribild Licensed to boost atazanavir and darunavir Likely that we can only use if ritonavir problems SAME DRUG INTERACTION ISSUES • Tivicay ABACAVIR + LAMIVUDINE + DOLUTEGRAVIR Trials! • 2 NRTI + boosted PI • Randomised to swicth to 2 NRTI + dolutegravir: – Immediately – After 48 weeks • ASK YOUR DOCTOR/NURSE/PHARMACIST ABOUT TRIALS EACH TIME YOU VISIT! Clinic response to current situation • Times are tough! • We are looking at everything we can to save money: – – – – Staff (number, roles) Tests Drugs Visits (frequency and type) Appointments • Where possible 6 monthly • Where possible face to face only once a year • In between: – – – – Email Phone ‘No news is good news’ (Specialist nurse) Blood appointments • You may be given a questionnaire • This is then scanned and reviewed, along with your results, at a ‘virtual’ appointment Home delivery • We know there have been problems! • Still saves a lot of money • Currently the reminders are not synced with your appointments • We are hoping to change this and there may be some teething problems…bear with us! Tests • CD4! – Only one a year if more than 350 – NEVER is more than 500…. PARTNER Study: HIV transmission risk through condomless sex if the HIV positive partner is on suppressive ART • Aim: – To evaluate the risk of within-couple HIV transmission (HT and MSM) during periods where condoms are not used consistently & the HIV+ partner is on suppressive ART Rodger et al. CROI 2014. O153LB. HIV negative partners: characteristics MSM couples (n=282) Heterosexual couples (n=445) M -ve (n=245) W-ve (n=240) 40 (32-47) 45 (37-50) 40 (34-46) 1.5 (0.5-3.5) 2.7 (0.6-6.9) 3.5 (0.7-10.6) 1.1 (0.7-1.9) 1.5 (1.0-2.0) 1.5 (0.9-2.0) Diagnosed with STI, % 16% 5% 6% CL sex with other partners, % 34% 3% 4% CL sex acts/year, median (IQR) 43 (18-79) 37 (14-77) 38 (14-71) Estimated total no. CL sex acts 16,400 14,000 14,000 At study entry Age, median (IQR) Yrs CL sex, median (IQR) During follow up Years in study, median (IQR) HIV positive partners: characteristics MSM couples (n=282) Heterosexual couples (n=445) M -ve (n=245) W-ve (n=240) 42 (36-47) 40 (34-46) 45 (40-49) 5 (2-11) 7 (3-14) 10 (4-15) Self-reported adherence ≥90% 97% 94% 94% Self report undetectable VL, % 94% 86% 85% CD4>350 cells/mm3, % 90% 88% 84% Having missed ART for more than 4 consecutive days, % 2% 7% 4% Diagnosed with STI, % 16% 4% 5% At study entry Age, median (IQR) Years on ART, median (IQR) During follow up Results • No transmissions! – Despite high levels of STI in HIV- MSM • If HIV+ partner not on ART would have expected a median of 86 transmissions at this interim 2 year analysis HIV transmission rate by sexual behaviour reported by the negative partner Rate of within couple transmission (per 100 CYFU) 0 0.2 0.4 0.6 0.8 1 1.2 10 year risk (%) of within couple transmission 0 2 Any sex (CYFU=894) Anal sex (CYFU=374) estimated rate/risk 95% confidence interval 4 6 8 10 PROUD Pre-exposure Option for preventing HIV in the UK: an open-label randomisation to an immediate or Deferred offer Aims of PROUD • To determine ‘real-life’ efficacy – When individuals know PrEP is effective – Mimic clinic routine as much as possible – Placebo alters behaviour, so non-placebo controls • Randomised: – Immediate PrEP vs deferred to 12m • Measures net benefit, behaviour + biology: – “...short daily diary…..monthly questionnaire and …. clinic appointment every three months” PrEP is coming….? • PROUD Study = MSM study in UK GU clinics • ‘High risk’ MSM randomised to: – Immediate PrEP (Truvada – FDC of 2 NRTI) – Delayed PrEP (12 months) • DSMB advised stopping the deferred arm October 2014 due to high rates of PrEP efficacy • PrEP licensed in the USA in 2012 • Not licensed in Europe BHIVA statement • “We welcome the news that we have made significant progress in efforts to prevent HIV in men who have sex with men, where ongoing transmission in the UK remains unacceptably high, and look forward to seeing the results when they are available. BHIVA, along with other key stakeholders, are working with NHS England to devise a policy to consider the future availability of pre-exposure prophylaxis, alongside existing measures to prevent infection, within the NHS in the future.” “On-demand” PrEP at sexual intercourse reduces risk of infection ANRS IPERGAY - France “On-demand” Truvada to be taken at the time of sexual intercourse February 2012 > 400 MSM at high risk of HIV infection Double-blind, randomised All participants received a package of preventative measures: • counselling • repeated HIV testing • screening & treatment for other STIs • HBV vaccination • condoms and gel “On-demand” placebo to be taken at the time of sexual intercourse • Un-blinded to counterpart DSMB of PROUD trial – Data demonstrates a significant difference in incidence between each arm The DSMB have recommended that all participants of IPERGAY now benefit from “on-demand” Truvada as soon as possible – Full results are expected in early in 2015 Press release. ANRS: A significant breakthrough in the fight against HIV/AIDS. 29 Oct 2014 Hepatitis C • We are still seeing A LOT • We have developed a leaflet • We have written for DirtyBoyz • We have updated our website • Talk to staff! • There are new drugs but guess what…………. ….we can’t use them yet!! Example: sofosbuvir Telemedicine Thank you! [email protected] Which one?
© Copyright 2026 ExpyDoc