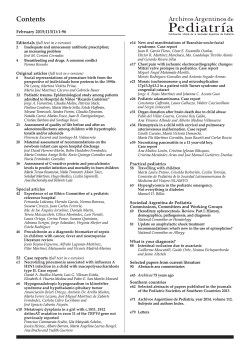
COGNITIVE IMPAIRMENT IN PEDIATRIC MULTIPLE SCLEROSIS PATIENTS IS NOT RELATED TO CORTICAL LESIONS P134 E. De Meo1, M. Rocca1,3, M. Copetti2, L. Moiola3, A. Ghezzi4, 1,2 M.3 Copetti,4 D.1,3 1,2 V. Martinelli,2 5, 1A. 6 P. Preziosa,1,2 M.A. Rocca,1,2M. E.Amato Pagani, M.E. Morelli, Dalla Libera, Falini , G. Comi , M. Filippi 3 G. Comi,2 M. Filippi.1,2 A. Falini, 1Neuroimaging Research Unit, Institute of Experimental Neurology, San Raffaele Scientific Institute, Vita-Salute San Raffaele University (Milano); 2Biostatistics Unit, IRCCS-Ospedale Casa Sollievo della Sofferenza (San Giovanni Rotondo-FG); 3Department of Neurology, San Raffaele Scientific Institute, Vita-Salute San Raffaele University (Milano); 4MS Centre, Gallarate Hospital (Gallarate-VA); 5Department of Neurology, University of Florence (Firenze); 6Department of Neuroradiology, San Raffaele Scientific Institute, Vita-Salute San Raffaele University (Milano). Table 3. Neuropsychological test scores (mean corrected values and SD) from patients with pediatric MS. INTRODUCTION In adult patients with MS, the use of double inversion recovery (DIR) sequences has consistently demonstrated an association between cognitive impairment and the number and volume of cortical lesions (CLs).[1] Correlative location-function studies have also shown that lesions located in strategic grey matter (GM) structures (for instance, the hippocampus) are associated with selective cognitive deficits.[2] The pivotal role of CLs for cognition in adult MS is also supported by a recent 5-year, large-scale, longitudinal study,[3] which found that the baseline volume of such lesions is one of the predictors of cognitive performance. Cognitive impairment affects a large proportion of pediatric MS patients,[4,5] with prominent involvement of attention, information processing speed, memory and executive functions, as it is the case of adult MS, but with an additional involvement of linguistic abilities.[4] Studies which have investigated the possible MRI substrates of cognitive deficits in pediatric MS have analyzed the contribution of white matter (WM) lesions, atrophy of the WM and/or GM or strategic CNS structures (e.g., the thalamus and corpus callosum) and microstructural damage to the major WM tracts.[5-8] An aspect that has not been investigated so far in these patients is the role of CLs in explaining the occurence of cognitive deficits. OBJECTIVES Pediatric CP MS patients Pediatric CI MS patients 97.5 (15.7) 96.8 (16.7) 98.0 (16.8) 99.4 (12.5) 100.0 (14.0) 97.2 (15.2) 95.7 (20.2) 91.7 (19.6) 101.2 (21.4) CDI 8.5 (5.7) 7.3 (4.9) 10.5 (6.8) FSS 26.8 (12.2) 26.4 (9.6) 24.7 (14.3) SRT-LTS 51.4 (12.3) 55.4 (7.8) 42.8 (15.7) SRT-CLTR 44.7 (14.7) 49.7 (10.8) 33.8 (16.4) SRT-D 9.7 (2.1) 10.2 (1.5) 8.6 (2.9) SRTm 35.2 (9.3) 38.4 (6.3) 28.4 (11.2) SPART 24.5 (4.4) 25.9 (2.8) 21.5 (5.6) SPART-D 8.7 (1.9) 9.2 (1.1) 7.6 (2.6) SPARTm 17.0 (3.7) 18.2 (2.9) 14.5 (4.1) 5.7 (0.6) 1.1 (1.9) 5.8 (0.6) 1.2 (2.0) 5.6 (0.7) 1.0 (1.8) SDMT 52.9 (12.7) 54.8 (12.2) 48.8 (13.5) TMT-A 41.4 (14.7) 38.5 (11.3) 47.7 (19.2) TMT-B 75.2 (42.4) 63.5 (24.0) 100.4 (60.8) Phonemic verbal fluency test 31.0 (9.3) 31.5 (9.6) 30.1 (8.8) Semantic verbal fluency test 22.9 (12.2) 25.2 (13.6) 18.0 (6.7) IPT 9.9 (0.2) 10 (0) 9.8 (0.4) PCT 29.8 (0.5) 29.8 (0.4) 29.7 (0.6) Token Test 34.8 (1.0) 34.8 (0.9) 34.7 (1.3) ODT 42.3 (4.6) 43.3 (3.1) 40.1 (6.5) Global IQ Verbal IQ Performance IQ Memory Abstract/conceptual reasoning (MCST) Aims of this study were: • To investigate the contribution of CLs, quantified using a DIR sequence, to cognitive impairment in pediatric MS patients; • To estimate the role of lesions in the WM as well as that of atrophy of brain WM and GM in the development of cognitive impairment. METHODS Completed categories Perseverative errors Attention/concentration Language Subjects: 41 relapsing remitting (RR) MS pediatric patients and 31 gender- and age-matched, healthy controls (HC). Neurological examination: Clinical evaluation, EDSS score rating; Neuropsychological assessment: Brief Neuropsychological Battery for Children (BNBC), standardized and validated for Italian pediatric MS. Patients with an abnormal performance in ≥ 2 tests were considered as cognitively impaired (CI).[9] MRI acquisition: (3.0 T Philips Intera scanner) • DIR sequence; • Dual-echo (DE) turbo spin-echo sequence; • 3D T1-weighted fast field echo (FFE) sequence. MRI analysis: • CLs were identified on DIR images (Figure 1); • T2 WM lesions (including those located juxtacortically) were identified on DE images; • T1 hypointense lesions were identified on 3D FFE images; • GM and WM hyperintense and WM T1 hypointense lesion volumes (LV) were measured using a local thresholding segmentation technique (Jim 5, Xinapse Systems); • Normalized brain volumes (NBV), GM (GMV) and WM (WMV) volumes were measured on 3D FFE scans using SIENAx software. Figure 1. Example of CL in a CP MS patient in A) DIR and B) T1-weighted sequences. (A) All pediatric MS patients Table 3 (B) Abbreviations: IQ=intelligence quotient; CDI=Children Depression Inventory; FSS=Fatigue Severity Scale; SRT-LTS=Selective Reminding Test-Long-Term Storage; SRT-CLTR=Selective Reminding Test-Consistent Long-Term Retrieval; SPART=10/36 Spatial Recall Test; SDMT=Symbol Digit Modalities Test; TMT-A/B=Trail Making Test A/B; SRT-D=Selective Reminding Test-Delayed; SPART-D=10/36 Spatial Recall Test-Delayed; MCST=Modified Card Sorting Test; IPT=Indication of Pictures Test; PCT=Phrase Comprehension Test; OD=Oral Denomination Test; SRTm=average score of verbal (SRT-LTS, SRT-CLTR, SRT-D) memory; SPARTm=average score of visuospatial (SPART, SPART-D) memory. Compared to CP patients, CI MS patients had significantly longer disease duration and lower NWMV, whilst they did not differ for age, EDSS, education, T2 LV, T1 LV, NBV and GMV (Tables 1 and 4). In pediatric MS patients, WMV was significantly correlated with the number of abnormal neuropsychological tests (r=-0.51, p=0.001). CLs were found in 3 (11%) CP and 2 (15%) CI MS patients (p=0.6). The number and volume of CLs did not differ significantly between CP and CI MS patients (Table 4). Table 4. summarizes the main neuroimaging findings from HCs, CP and CI pediatric MS patients. Pediatric HC Pediatric MS patients p* value Pediatric CP MS patients Pediatric CI MS patients p* value Mean T2 LV (SD) [ml] - 4.8 (5.6) - 4.3 (5.7) 6.0 (5.7) 0.2 Mean T1 LV (SD) [ml] - 2.9 (3.3) - 2.5 (2.8) 3.9 (4.2) 0.2 Median Number of CLs (range) - 0 (0 - 3) - 0 (0 - 3) 0 (0 - 2) 0.9 Mean CL volume (SD) [ml] - 0.02 (0.05) - 0.02 (0.05) 0.01 (0.03) 0.8 Mean NBV (SD) [ml] 1713 (88) 1646 (79) 0.003 1665 (69) 1608 (87) 0.06 Mean GMV (SD) [ml] 860 (70) 825 (57) 0.03 832 (57) 811 (58) 0.3 Mean WMV (SD) [ml] 853 (49) 821 (47) 0.04 832 (46) 805 (47) 0.01 Table 4 Statistical analysis: • Between-group comparisons of demographic, clinical and conventional MRI variables: Pearson chisquare test, Fisher exact test and non-parametric Mann-Whitney U test, as appropriate; • Between-group comparisons of CL number: negative binomial regression model; • A p-value<0.05 was considered for statistical significance. *Mann-Whitney U test. Abbreviations: CI=cognitively impaired; CP=cognitively preserved; EDSS=Expanded Disability Status Scale; LV=lesion volume; CL=cortical lesion; NBV=normalized brain volume; GMV=grey matter volume; WMV=white matter volume. RESULTS CONCLUSIONS Table 1. shows the main demographic and clinical characteristics of the study subjects. Table 1 Number of subjects Girls / Boys Mean age (SD) [years] Median disease duration (range) [years] Pediatric HC Pediatric MS patients p* value Pediatric CP MS patients Pediatric CI MS patients p* value 31 41 - 28 13 - 19/11 27/14 0.3 21/7 6/7 0.07 14.9 (3.5) 15.2 (2.5) 1 14.9 (2.3) 15.7 (2.7) 0.2 - 1.2 (0.12-8.1) - 1.05 (0.1-3.1) 3.1 (0.3-8.1) 0.02 *Mann-Whitney U test. Table 2. summarizes neuropsychological performance from CP and CI pediatric MS patients. All pediatric MS patients Pediatric CP MS patients Pediatric CI MS patients 34.1 % 7% 92.3 % Language 39 % 25 % 69.2 % Attention 12.2 % 3.6 % 30.8 % Visual and verbal memory 34.1 % 7% 92.3 % Table 2 Visual and verbal memory CLs do not contribute to explain the occurrence of cognitive impairment in pediatric MS patients. The frequency of CLs in pediatric MS patients is much lower (12% in this study) than that usually reported in adult patients with MS, including those with clinically isolated syndromes[10] or radiologically isolated syndromes,[11] who have been reported to show CLs in nearly 40% of the cases.[10, 11] Atrophy of the WM was the only MRI measure capable to distinguish CI from CP pediatric MS patients. Conversely, the two groups did not differ for T2 LV, T1 LV, and GMV. In line with the pattern of cognitive dysfunction reported in previous studies,[4, 5] we found that our patients had a prominent involvement of spatial and verbal memory abilities, language, attention and concentration. All of this indicates that our sample is representative of the more general population of patients with pediatric MS. Combined with the recent demonstration that structural damage to the WM is one of the most important substrates of cognitive deficits in pediatric MS,[5] these results deepen our understanding of the pathogenesis of CI in patients with pediatric MS. Longitudinal studies are now warranted to define whether the contribution of WM damage to cognitive impairment reflects a deficit of maturation and myelination of CNS structures in pediatric MS patients. REFERENCES 1. 2. 3. 4. Calabrese M et al., Nat Rev Neurol 2010; Roosendaal SD et al., J Magn Reson Imaging 2008; Calabrese M et al., Brain 2012; Amato MP et al., Neurology 2008; 5. 6. 7. 8. Rocca MA et al., Neurology 2014; Till C et al., Arch Clin Neuropsychol 2012; Bethune A et al., J Neurol Sci 2011; Till C et al., Neuroreport 2011; 9. Portaccio et al., Mult Scler 2009; 10. Calabrese M et al., Arch Neurol 2007; 11. Giorgio A et al., Neurology 2011; This work has been partially supported by a grant from Italian Ministry of Health (GR-2009-1529671).
© Copyright 2026 ExpyDoc