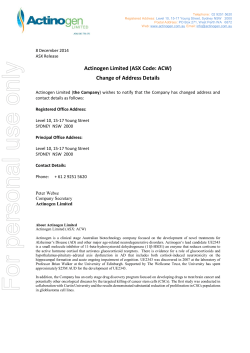
COMMAND: A Phase 2 Randomized, Double-blind, Placebo-Controlled, Multicenter Study of Defactinib as Maintenance Therapy in Subjects with Malignant Pleural Mesothelioma which has Not Progressed on at least 4 Cycles of Pemetrexed/Platinum Therapy Paul Baas , Dean Fennell , Richard J. Gralla , Hedy Kindler , Lee M. Krug , Anna K. Nowak , Lawrence H. Schwartz , Mitchell 8 8 Keegan , Joanna C. Horobin 1 2 3 4 5 6 7 1. The Netherlands Cancer, Amsterdam NL, 2. University of Leicester, Leicester UK, 3. Albert Einstein College of Medicine, Bronx, NY USA, 4. University of Chicago, Chicago, IL USA, 5. Memorial Sloan-Kettering Cancer Center, New York, NY USA, 6. University of Western Australia, Perth, AU, 7. Columbia University College of Physicians and Surgeons, New York USA, 8. Verastem, Needham, MA USA BACKGROUND COMMAND STUDY DESIGN Defactinib (VS-6063) • Defactinib targets cancer stem cells (CSCs) through the inhibition of focal adhesion kinase (FAK) • CSCs are tumor cells resistant to standard therapies and capable of seeding new tumors resulting in tumor recurrence and metastasis (see Fig 1) • SOC agents used for the treatment of malignant pleural mesothelioma (MPM) have been shown in pre-clinical models to increase the proportion of CSCs (see Fig 2) • The PK and toxicity profile of defactinib has been previously characterized in Phase 1 studies in patients with advanced solid tumors • ~50% of patients with MPM have loss or low levels of the tumor suppressor gene encoding the moesin-exrin-radixin-like protein (merlin) • Merlin regulates FAK and plays a role in cell adhesion, invasion and cell motility • Merlin-low mesothelioma cell lines are more sensitive to defactinib than merlin-high cell lines in vitro and in vivo (see Fig 2) Figure 1: Targeting Cancer Stem Cells as Maintenance Therapy Problem: Problem: Problem: Current cancer treatments Current Currentcancer cancer treatments treatments Inial tumor Goal: Inialtumor tumor Inial Inial tumor CSC Drugs CSC Drugs durable MoreMore durable clinical clinical More durable response response clinical Tumor reducon Tumor reducon CSCs butbut CSCs areare Tumor reducon enriched enriched response but CSCs are enriched Figure 2: Defactinib Kills Cancer Stem Cells and is More Potent in Merlin-low Cell Lines 600 400 400 200 600 400 200 20 DM D P M S Pr remSO O em e et trex re e xe d Ci d sp Ci la tin Gsepl a m Ge ctiint m cit abin Vaib e noin Vi ree no lb in re e lb iVn Se60 VS 63 -6 06 3 20 200 20 B 100 C C Merlin-High Mero-25 Merlin-High Mero-25 H2452 max H2452 H226 max H226 MSTO-211H MSTO-211H H28 Mero-25 Merlin-High H score H28 MM87H2452 H score or MM87 max Mero-14 or H226 Mero-14 Mero-41 MSTO-211H Mero-41 Mero-83 C 125 100 75 125 75 50 100 50 25 75 25 0 0.0010 0.01 50 0.001 0.1 1 VS-60630.1 (mM) 0.01 1 VS-6063 (mM) 25 0 0.001 10 0.01 0.1 1 VS-6063 (mM) 100 10 10 H28 Mero-83 MM87 100 Mero-14 Mero-41 Mero-83 min Merlin-Low or Pr SO em et re xe d Ci sp la tin Ge m cit ab in Vi e no re lb in e VS -6 06 3 CT Scan CT Scan ≥ 4 cycles ≥ 4 cycles PR/SD 350-400 PR/SD 350-400 Planum/Alimta Planum/Alimta ≥ 4 cycles Planum/Alimta PR/SD 350-400 0 Key Endpoints CT Scan 24 0 02 2 4 6 weeks 46 8 weeks PFS OS6 8 QoL weeks PlaceboPlacebo BID BID Placebo BID MerlinMerlin High High Merlin High VS-6063VS-6063 400mg BID 400mg BID VS-6063 400mg BID H score Key Exclusion Criteria • History of upper GI bleed, ulceration or perforation • Major surgery within 28 days • Gilbert’s syndrome • Serious active infection • History of malignancy within 5 years STUDY STATUS Enrolling now in many countries worldwide min Merlin-Low 100 (A) Inhibition of Aldefluor‑positive mesothelioma CSCs by defactinibMerlin-Low in contrast to induction by chemotherapy. (B) Cell viability analysis of merlin high (green) or merlin low (blue) MPM cell lines treated with defactinib. (C) Immunohistochemistry for merlin expression in MPM patient biopsies. An H-score is used for stratifcation. DM Aldefluor Posve CSCs (% of Control) 800 600 125 Cell Viability (%) 800 Aldefluor Posve CSCs Aldefluor Posve CSCs (% of Control) (% of Control) A 800 BB Cell Viability (%)Cell Viability (%) AA CT Scan Key Inclusion Criteria • Histological proof of MPM (and Merlin status) • Measurable or evaluable disease per RECIST v1.1 • One prior regimen (≥4 cycles) pem/cis or pem/carbo with a documented ongoing response (PR or SD) • KPS ≥70% Recurring tumortumor Recurring Chemobut CSCs survive CSC Drugs Chemo Goal: Recurring tumor but CSCs survive Chemo Goal: • Central review of CT scans KEY ENTRY CRITERIA Tumor reducon Tumor reducon Tumor reducon but CSCs survive Inial tumor Inial tumor • Paents strafied by tumor merlin status, • Paents strafied by assessed by IHC tumor merlin status, Placebo BID • Treatment unl • Paentsassessed strafied by by IHC Placebo BID progression Treatment tumor• merlin status,unl Merlin Low • Interim analysis at 128 assessedprogression by IHC Merlin Low Placebo BID progression events • Interim analysis at 128 • Treatment unl VS-6063 400mg BID progression • Centralevents review of CT progression VS-6063 400mg BID Merlin Low • analysis Central review • Interim at 128 of CT scans Key progression events scans VS-6063 400mg BID CT Scan CT ScanKey Endpoint min OBJECTIVES Primary Efficacy Objectives • Progression free survival • Overall survival Secondary Efficacy Objectives • Quality of Life using LCSS-Meso • Objective response rate Exploratory Efficacy Objectives • Determine time to new lesion • Evaluate the relationship of defactinib PK and outcome • Population PK Presented at the 2014 iMig annual meeting 21-24 October in Cape Town, South Africa SUMMARY • Study is open and actively accruing at multiple centers • Accrual is expected to be completed in second half of 2015 for PFS endpoint • IHC assay has been validated for the determination of merlin in patient biopsies • For additional information see www.COMMANDmeso.com Clinical Trial Registry Number NCT01870609 PFS OS QoL 8
© Copyright 2026 ExpyDoc