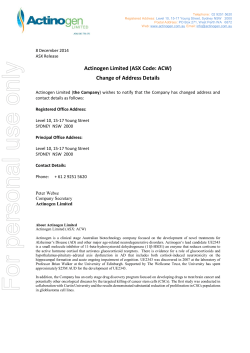
VICE-DIRECTION OF TRANSLATIONAL RESEARCH MOLECULAR PATHOLOGY PROGRAMME | SteM ceLLS AnD cAnceR GRoUp STEM CELLS AND CANCER GROUP Christopher Heeschen Group Leader Staff Scientists Alexandra Aicher (since February), Susana García, Bruno Sainz, Patricia Sancho Post-Doctoral Fellows Maria Azevedo (until September), Anamaria Balic (until July), Jorge Dorado (until June), Sara Trabulo, Yolanda Sánchez (until September) Graduate Students Álvaro Castells (since November), Michele Cioffi, Anja Fries (since September), Irene Miranda, Marina Roy (since August), Alejandra Tavera (since October), Sladjana Zagorac Technicians Sonia Alcalá, Emma Burgos, Magdalena Choda (since September), Catarina L. Reis, Marianthi Tatari (since May), Mireia Vallespinos (since May) Visiting Scientists Patrick C. Hermann (until October), Morten Draeby Sorensen Christopher Heeschen DEU Alexandra Aicher DEU Susana García ESP Patricia Sancho ESP Sara Trabulo PRT Álvaro Castells ESP Michele Cioffi ITA Anja Fries USA Irene Miranda ESP Marina Roy ESP Alejandra Tavera MEX Sladjana Zagorac SRB Sonia Alcalá ESP Emma Burgos ESP Magdalena Choda POL Catarina L. Reis PRT Marianthi Tatari GRC Mireia Vallespinos ESP Morten Draeby Sorensen DNK OVERVIEW With the availability of more sophisticated model systems and technologies it has now become evident that cancer heterogeneity is even greater than anticipated from the multiple genetic alterations, but it is also driven by the phenotypic and functional heterogeneity and plasticity within each subclone of the tumour. Indeed, pancreatic cancer stem cells (CSCs) represent a subset of cancer cells, for which we, and others, have provided conclusive evidence that these cells represent the root of the disease by giving rise to all the differentiated progenies within each cancer subclone (FIGURE 1). Scientific RepoRt 2013 “ Our research should ultimately allow us to develop novel multimodal therapies to eliminate both CSCs, as the root of pancreatic cancer, and their differentiated progenies. Targeted delivery of new therapies in combination with advanced imaging technologies will be achieved by nanoparticle technology and tested in well-designed clinical trials.” Even more important, from a clinical perspective, these cells are driving the metastatic behaviour of pancreatic cancer and are the putative source for disease relapse. Therefore, CSCs are responsible for the intraclonal heterogeneity of the tumour and represent a crucial component for the development of novel treatments. Noteworthy is the fact that CSCs do not represent bona fide stem cells based on most stringent criteria, nor do they necessarily arise from tissue stem cells. Instead, CSCs have acquired certain features of stem cells. While CSCs and their differentiated progenies demonstrate an identical genetic ground state with respect to genetic 94 SpAniSH nAtionAL cAnceR ReSeARcH centRe, cnio alterations, as demonstrated by single-cell implantation experiments, CSCs exhibit distinct gene expression profiles that share modules with pluripotent stem cells. Most of the genes involved in generating induced pluripotent stem cells (iPS cells) − such as Nanog, Oct3/4, Klf4, and Sox2− have been linked to cancer and are strikingly overexpressed in the pancreatic CSC compartment. 95 VICE-DIRECTION OF TRANSLATIONAL RESEARCH MOLECULAR PATHOLOGY PROGRAMME | SteM ceLLS AnD cAnceR GRoUp RESEARCH HIGHLIGHTS Figure 2 CAM-PaC strategy. Gathering of (pre-) clinical, histopathological, RNAseq, and metabolic data. Data integration using a combination of bioinformatics and tailored shRNA library screens for self-renewal, metastasis and resistance. Target screen using established in vitro models. Target validation using RNAi mice. Eventually, we want to identify novel therapeutic targets and predictive biomarkers, which would then be tested in innovative early-phase clinical trials. Figure 1 Cancer Stem Cell (CSC) concept. Although the origin of CSCs still remains elusive for most cancer entities and may actually vary between patients, distinct populations of CSCs have already been identified (once the tumours have been formed). CSCs are defined by their unlimited self-renewal, the capability to recapitulate the tumour heterogeneity (differentiation) and their exclusive in vivo tumourigenicity. CSCs are not a single population of uniform cells; rather, they undergo evolution through the acquisition of genetic and epigenetic alternations. Also, the tumour microenvironment can induce dramatic changes in their phenotypic characteristics. For example, a distinct subpopulation of migrating CSCs, identified by additional CXCR4 expression, can be detected in the invasive front in the pancreas as well as in the circulating blood. Detection of these circulating CSCs could serve as prognostic and predictive biomarkers and, even more importantly, their prospective isolation as a liquid biopsy should eventually provide non-invasive access to metastatic CSCs. ∞ ∞ Targeting the metabolic Achilles heel of human pancreatic CSCs CSCs, actually underwent rapid apoptotic death due to energy crisis. Epidemiologic studies have suggested that diabetes mellitus, particularly type II, is associated with enhanced risk for pancreatic cancer. Strikingly, in a retrospective analysis, oral administration of metformin in patients with diabetes mellitus type II was found to be associated with a reduced risk for developing pancreatic cancer as well as better outcome in patients with established pancreatic cancer. When evaluating metformin for the treatment of pancreatic cancer in large preclinical studies, we found that the heterogeneous populations of cancer cells harboured in primary human pancreatic cancer tissues differed strikingly in their response to metformin depending on their level of stemness. While the bulk of more differentiated cancer cells reacted to metformin treatment with cell cycle arrest, a subset of cells with distinct stemness features, namely Our data demonstrate that metformin virtually exhausted the CSC fraction, but are also consistent with the notion that non-CSCs do not replenish the pancreatic CSC pool after termination of metformin treatment. Further metabolic studies have suggested that pancreatic CSCs actually bear a highly mitochondrial-dependent metabolic profile, which is in striking contrast to normal stem cells, but also distinguishes them from the bulk cancer cells. Metformin is slowly accumulated 1000-fold within mitochondria and directly inhibits Complex 1 (NADH dehydrogenase), thus interfering with this proton gradient across the inner mitochondrial membrane. Subsequent alteration in the electron transport chain and oxidative phosphorylation appear to be particularly lethal for CSCs. Therefore, drugs such as metformin that target the oxidative mitochondrial PUBLICATIONS Sainz B Jr, Heeschen C. (2013). Standing out from the crowd: cancer stem cells Scientific RepoRt 2013 ∞ in hepatocellular carcinoma. Cancer Cell 23, 431-433. Hermann PC, Heeschen C (2013). Metastatic Cancer Stem Cells--Quo Vadis?. ∞ Clin Chem 59, 1268-1269. Trakala M, Fernández-Miranda G, Pérez de Castro I, Heeschen C, Malumbres M (2013). Aurora B prevents delayed DNA ∞ replication and premature mitotic exit by repressing p21 (Cip1). Cell Cycle 12, 1030-1041. Hermann PC, Trabulo SM, Sainz JrB, Balic 96 metabolism represent powerful therapeutic tools for attacking the CSC pool. Launching an interdisciplinary research programme to identify novel targets against CSCs For many human malignancies, large-scale genomic, transcriptomic and, to a somewhat lesser degree, proteomic analyses have been instrumental in establishing a comprehensive catalogue of molecules that are altered in their structure and/ or abundance in bulk tumours. Far less developed are concepts and methods for the integration of data from CSCs and their progenies, and to perform systematic interrogation of gene functions for CSC features in order to differentiate ‘driver’ alterations − which directly contribute to tumourigenicity and/or metastasis − from “passenger” alterations, which have minimal or no influence on CSC biology. A, Garcia E, Hahn SA, Vandana M, Sahoo SK, Tunici P, Bakker A, Hidalgo M, Heeschen C (2013). Multimodal treatment eliminates cancer stem cells and leads ∞ to long-term survival in primary human pancreatic cancer tissue xenografts. PLoS One 8, e66371. Lonardo E, Cioffi M, Sancho P, Sanchez- SpAniSH nAtionAL cAnceR ReSeARcH centRe, cnio Therefore, the goal of our new pan-European project CAMPaC is to functionally interrogate transcriptomic data from a large set of primary human pancreatic CSCs in order to systematically identify these driver genes/pathways (FIGURE 2). This will be achieved by tailored shRNA screening (~500 pre-specified genes). The obtained shortlist of genes/pathways (~20 per functional feature) will then be comprehensively characterised and, if indeed of crucial functional relevance for the CSC phenotype, further validated as novel CSC targets for therapeutic intervention. Eventually, a unique collection of pre-selected and pre-characterised CSC candidate genes will be selected for systematic functional characterisation using RNAi mouse models in combination with novel genetically engineered mouse models of pancreatic cancer. The latter will allow for the independent temporal control of up to four initiating genetic events (e.g. 1st hit: KrasG12D/+, 2nd hit: Tp53R172H/+, 3rd hit: DPC4 shRNA) in a postnatal setting and should more accurately reflect human disease. s Ripoll Y, Trabulo SM, Dorado J, Balic A, Hidalgo M, Heeschen C (2013). Metformin targets the metabolic achilles heel of human pancreatic cancer stem cells. ∞ PLoS One 8, e76518. Garcia-Silva S, Frias-Aldeguer J, Heeschen C (2013). Stem cells & pancreatic cancer. Pancreatology 13, 110-113. 97
© Copyright 2026 ExpyDoc