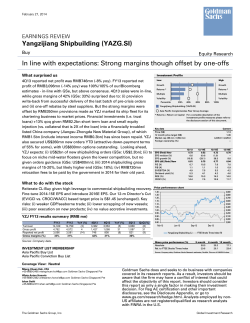
Fortnightly Thoughts March 6, 2014 Issue 70 Healthcare innovation on the mend? From the editor: In this edition we examine two key themes; the improving pace of innovation and how to pay for the rising demand for, and price of, healthcare. We interview three experts on these issues and have pieces from our global healthcare analysts. Healthcare is clearly different from most industries in many ways; the degree of regulation, the specialist knowledge requirement and the exposure to governments as customers, are all unusually high. But in some ways, pharma, in particular, is similar to other high return industries. It always needs to find new products and management’s cash allocation decisions, as they seek to refresh and replenish portfolios either organically or through acquisitions, are crucial. Finding structurally growing patient pools or products that are superior in capability has produced stellar performance in terms of total shareholder return - Bristol-Myers, Shire, Novo Nordisk and Roche are all well positioned here. Lots of themes touch healthcare – demographics, middle class lifestyles (DM and increasingly EM), the role of government, the importance of IP, dominators buying disruptors and the ubiquity of technology. What’s inside Healthy returns Sector CROCI levels versus volatility, GS European coverage 8% Technology Standard deviation of CROCI 2003-2017E 7% Oil Services 6% Mining 5% Media Steel 4% 3% 2% 1% Autos Construction Oil Business Trans Svcs. and Trav Aerospace Machinery Retail Consumer Products Chemicals Utilities Telecoms 0% 5% 10% But for much of this edition, we focus on innovation as we look at growing disease areas e.g. Alzheimer’s and new treatment solutions e.g. immunotherapy, genomics, 3D printing, stem cells. Our interviews are with experts on cancer and the US pharma industry – Dr. Peter Bach of Memorial Sloan-Kettering, on the role of government and the UK healthcare system - Sir Michael Rawlins and Sir John Chisholm who chairs Genomics England. 15% MedTech Pharma 20% 25% 30% Average market cap weighted CROCI 2003-17E Source: Goldman Sachs Global Investment Research. Hugo Scott-Gall [email protected] +44 (20) 7774 1917 Goldman Sachs International Sumana Manohar, CFA [email protected] +44 (20) 7051 9677 Goldman Sachs International Innovation on the mend?: Our lead article 2 Change is the only constant: European pharma team on emerging therapeutic areas 5 Interview with…Sir John Chisholm: Executive Chairman of Genomics England 8 Genomics: Changing pharma: Isaac Ro 10 Interview with…Dr. Peter Bach: Director, Memorial Sloan-Kettering Cancer Center 12 Cancer immunotherapy is paradigm changing: Jami Rubin 14 Interview with…Sir Michael Rawlins: President, UK’s Royal Society of Medicine 16 Making the case for stem cells: Andrea Chong 18 China: Insurance key for healthcare reform: Wei Du 20 The 3D printing revolution: Veronika Dubajova 22 Goldman Sachs does and seeks to do business with companies covered in its research reports. As a result, investors should be aware that the firm may have a conflict of interest that could affect the objectivity of this report. Investors should consider this report as only a single factor in making their investment decision. For Reg AC certification and other important disclosures, see the Disclosure Appendix, or go to www.gs.com/research/hedge.html. Analysts employed by non-US affiliates are not registered/qualified as research analysts with FINRA in the U.S. The Goldman Sachs Group, Inc. Goldman Sachs Global Investment Research Fortnightly Thoughts Issue 70 Healthcare innovation on the mend? An expanding opportunity set, rising costs for constrained governments as well as consumers, new enabling technologies and signs of a fresh wave of innovation, together place the healthcare industry at a fascinating juncture. These factors, taken in the context of the large revenue pools and stable (and often high) returns that the industry has to offer should make it ripe for disruption. In the pages that follow, our global healthcare analysts delve into where we see opportunities for disruptive innovation and who is driving it, while in this essay, we focus on what the problem is, why it needs to be resolved and how we can identify genuine winners in the industry. Generalist practitioner The healthcare complex ticks many of our key thematic boxes – changing consumer habits (food and wellness), dominators versus disruptors, the ubiquity of technology (data, analytics and devices), the role of governments and demographics, with the latter two at the heart of the healthcare conundrum. About 60% of global population growth by 2040 is expected to come from those older than 54 years, who on average spend double on healthcare than the rest of the population (in the US). So the demand for drugs and services is set to rise further. Compounding that is the rising per capita cost of healthcare, particularly pharmaceutical drugs; the inflation adjusted expenditure per person has risen in most major economies over the last decade. Real growth Annual average growth in expenditure on health and pharmaceuticals, in real terms, 2000-2011 10% physicians, hospitals, long-term care etc. In the US, where private participants still dominate these parts of the value chain (except medicare/ medicaid), the last few years have been marked by consolidation. Independent hospitals are becoming parts of larger chains driven by reimbursement pressures, higher penalties for low-quality care and economies of scale. Front-end pharmacies have consolidated too (Walgreens, Rite Aid and CVS account for 70% of the drug retail market) and now have better negotiating power with their suppliers. For instance, almost all front-end retailers in the US buy generics directly from drug manufacturers, disintermediating wholesale distributors (which have similarly been through a consolidation phase). Such a competitive environment has brought down costs to an extent and there might be potential for more efficiency, via automation and technology, but there isn’t much juice left. The median operating profit margin for all the listed healthcare providers in the US was 8% in 2012 versus over 20% for pharmaceuticals and medtech. In other words, despite accounting for c.50% of total revenues in the industry, healthcare providers generate less than a quarter of the operating profits (versus pharma – 32% of revenue and 50% of EBIT in 2012). Of course in most of the other DMs, healthcare delivery is typically provided by governments, and reforming labour costs - wages and headcount - is politically, a difficult pill to swallow (the UK’s NHS was the 5th largest employer in the world in 2012). And so here too, policy makers tend to focus on drug producers to reduce costs. Pharma is a sweet spot % of total listed healthcare industry, by sector, 2012 Pharmaceuticals Biotechnology Healthcare Providers Medical Equipment Medical Supplies 8% Healthcare Employees Pharmaceutical drugs 6% Operating profit 4% 2% Sales 0% R&D Italy Switz. France Denmark Germany Norway Australia Canada US Sweden Japan Spain Finland UK Korea Netherlands -2% Source: OECD. Market Value 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% Source: Datastream. More effective drugs, targeted treatments and solutions for rare conditions or previously terminal diseases represent much progress made by the industry, but they naturally come at a greater cost, which in most DMs is borne by governments (>60% of total healthcare spend in the OECD). Over the last decade, the proportion of government outlays spent on healthcare has risen in almost every advanced economy, with some of the biggest shifts coming in Netherlands, Switzerland and China. And the future looks no different. Given that demographic (healthcare demand) trends are essentially irreversible in the medium term in many of these economies, governments have few options to ease the healthcare burden – increase funding (either raise taxes or reallocate funds from other, more productive areas) or decrease spending (pay less or pay for fewer treatments). Cost cutting difficult Where can costs be cut? To answer that, we need to first look at where healthcare dollars are being spent. Drugs and medical goods account for about 20% of total expenditure in DMs, with the rest going to healthcare delivery and services – logistics, pharmacies, Goldman Sachs Global Investment Research Why are returns so high for big pharma? Pharma provides one of the most attractive cash return profiles on a market-cap weighted basis (second only to technology for 201417E for our European coverage) which reflects its innovationintensive nature; i.e. high-returns are driven by monopolistic pricing which are justified by the significant levels of risk capital necessary for bringing a drug to market, which in most cases takes several years. This in itself does not preclude new, small entrants (e.g. Innate Pharma) from competing with the incumbents. But bigger companies that have invested in a portfolio of drugs, often in different stages of development (i.e. diversification) are better placed to sustainably manage this R&D risk, and the associated regulatory hurdles over the long run. Additionally, big pharmaceutical companies have also consistently used their large balance sheets to acquire innovation; large cap pharma companies in Europe have spent about $300 bn on M&A in the last 10 years compared to $390 bn on R&D. The biotech space is a case in point. Roche-Genentech, Sanofi-Genzyme, Bristol-Myers-Mederex are among the many examples of in this context. 2 Fortnightly Thoughts Issue 70 This brings us to the unique challenge for pharmaceutical companies. Unlike broader, successful consumer product companies that can rely on the strength of their brands to generate revenues for an extended period of time, pharma companies (even the ones with the best drugs) have a finite number of years to recoup their investment given the patent cycle, which means that there is a constant need to renew their product pipeline. Pharma management teams are then particularly important cash allocators, taking cash flow from mature assets and redeploying into organic (R&D) or inorganic (M&A) innovation. Shire is an example of a serial acquirer, which has acquired nearly every product it sells today. Purchasing skills Shire expenditure on R&D and M&A, US$ mn 5,000 4,500 R&D expense M&A/inlicense payment 4,000 3,500 3,000 2,500 2,000 1,500 1,000 500 0 2007 2008 2009 2010 2011 2012 2013 *Caveats: 1. M&A payments only included for where data is disclosed, 2. Payments are the maximum gross amount that would be paid out as per agreement, and 3. 2007 New River deal was funded by raising debt and equity financing Source: Goldman Sachs Global Investment Research. Cash managers This constant need to replenish their product portfolios also perhaps explains why despite having relatively high and stable cash returns on an industry level, individual pharma companies have an unusually short duration of returns leadership versus other sectors in our coverage i.e. top-quartile cash return (Q1 CROCI) generating companies remain Q1 for an average of 6.6 years compared to a cross-sector average of 7.3 years. But there are exceptions of course. Globally, Novo Nordisk, Shire and Roche are the only three large cap pharmaceutical companies which have generated above sector-median CROCI since 2009 and our analysts expect them to continue to do so at least until 2017. Consistent with that, the three stocks also have yielded very high market relative total returns over the past decade with Novo in particular standing out (>800% since 2001). What do they have in common? They all tick at least one of the following boxes – growth in patient pool size, higher relative product capability or scale (for meaningfully lower cost of production) and therefore a dominant position. So, what lies ahead? On page 5, Keyur Parekh identifies where patient pools are growing (spoiler alert: Alzheimer’s, heart failure, new therapies for cancer), noting that a first mover in these areas could have a significant advantage. A case in point here is BristolMyers, which has adapted its portfolio to include immunotherapy, an emerging therapeutic area of oncology, which should, in our analysts’ point of view, improve its longer-term positioning. Spotting the right growth market and backing the right projects (or buying the right targets) beats the fade and allows for superior earnings Goldman Sachs Global Investment Research growth. To generate alpha, identifying the companies that get this right has mattered more than near-term valuation. To make this point in a different way, if we consider Novo Nordisk at the start of 2002, the starting multiple that we would have had to pay for it to just to match the market in the next decade would have been 63x 2003 EPS. Earnings power is what matters most. Is pricing power invincible? All else being equal, in an industry with high entry barriers (patents), companies that dominate their respective markets (such as types of cancer, vaccine, insulin, biologics) should enjoy excellent pricing power. And this has contributed to drug price inflation, perhaps most evidently in the US. But how does this reconcile with the need to reduce healthcare costs? In our interview with Sir Michael Rawlins on page 16, he speaks about the NICE model in the UK which looks at assessing the price of a drug based on the incremental benefit it provides to the user; essentially a monopsony market where the price is determined by the value of the product rather than the cost of its manufacture. On page 12, we speak to Dr. Peter Bach who argues for a similar model in the US, but notes that with a mostly private company led industry, valuebased pricing will be much harder to achieve. The vital signs of the next innovation wave Innovation and new revenue opportunities go hand in hand and there are a number of new treatment areas that show that innovation is accelerating after a relatively dormant decade. On page 14, Jami Rubin writes about the potential in immunotherapy to treat cancer, which works by harnessing the immune system to fight off cancer cells rather than the traditional treatments which target cancer cells themselves. On page 10, Isaac Ro notes the significant cost improvements made in gene sequencing technology and how it can revolutionise diagnosis, pre-diagnosis and treatment efficacy. On page 18, Andrea Chong highlights the progress made in stem cell research and the potential use in several areas such as cardiovascular conditions, orthopaedic diseases etc. And on page 24, Veronika Dubajova delves into the use of 3D printing technology for customised solutions in medtech and what it could mean for prosthetics and artificial organs in the future. These developments are all exciting and can potentially improve the length and/or quality of human lives considerably. But are they all necessarily cost-effective? In an industry that competes primarily on capability rather than cost, given the price inelastic nature of its products, it is not surprising that many of these innovations are focused on providing better (albeit relatively expensive) solutions. Given that private-sector innovators and governments have a different and diverging set of priorities (profits vs. costs), the solution may well lie in the direction of a combined effort between the two. We interview Sir John Chisholm of Genomics England (initially funded by the UK government) on page 8 who argues that better genetic data can help patients identify the particular variation of a disease, such as cancer, they are afflicted with, which should in turn enable them to get more appropriate, targeted treatment much earlier than was previously possible. This should reduce the lifetime cost of the treatment, which in the longer run is beneficial for payers. But at best, this feels like we are the end of the beginning and certainly not at the beginning of the end in the quest to balance insatiable demand for healthcare solutions and the rising costs associated with it. 3 Fortnightly Thoughts Issue 70 Six charts to nurse Almost unparalleled pricing power Dominant demand for labour YoY growth in pricing (sales/ext. unit growth) of top 200 generics and top 200 brands (US$) launched pre-2010 10 fastest growing occupations in the US which employ more than 100,000 people, % change in jobs expected between 2012 and 2022 Generics Branded Personal care aides 20% Home health aides 15% Physical therapist assistants and aides 10% Medical secretaries Health teachers, postsecondary 5% Nurse practitioners 0% Dental hygienists Market research analysts, marketing specialists -5% Cement masons, concrete and terrazzo workers Misc. health technologists and technicians 5% 10% 15% 20% 25% 30% Source: BLS. Growth everywhere The State of affairs Average consumption of different drugs across OECD countries, defined daily dosage per 1,000 people Expenditure on health by type of financing, 2011 2000 Private out-of-pocket 2011 Private insurance General Government 35% 40% 45% Social Security Other Mexico 0% Source: IMS Health, Goldman Sachs Global Investment Research. China Q3 2013 Q2 2013 Q1 2013 Q4 2012 Q3 2012 Q2 2012 Q1 2012 Q4 2011 Q3 2011 Q2 2011 Q1 2011 Q4 2010 -10% 50% 100% 400 90% 350 80% 300 70% 60% 250 50% 200 40% 150 30% 100 20% 10% 50 Source: OECD. India Russia Brazil S.Korea Spain Switz. Italy Finland Sweden Japan US UK Norway Antidepressants Denmark Antidiabetics Germany Anticholesterols N.Zealand Hypertension France Netherlands 0% 0 Source: OECD, World Bank. Booming boomers Average annual expenditure on healthcare by age and as a % of total after tax income, US Health insurance Medical services Drugs Medical supplies CAT scans per 1,000 population, 2011 (or nearest year) 300 As a % of income, RHS $5,500 More checking 16% $5,000 14% 250 $4,500 12% $4,000 $3,500 200 10% 150 $3,000 8% $2,500 6% $2,000 $1,500 4% $1,000 100 50 2% $500 0 $0 0% Under 25 years 25-34 years 35-44 years 45-54 years 55-64 years Source: BEA. Goldman Sachs Global Investment Research 65-74 years 75 years and older Canada France Germany CAT exams per 1000 population (2011 or nearest year) United States OECD average Source: OECD. 4 Fortnightly Thoughts Issue 70 Change is the only constant The only constant in the ever-changing world of pharma R&D is innovation (admittedly less productive at times than others). But, we would suggest that identifying future dominance and /or early movers represents a significant investment opportunity. Roche’s EV has risen from c.US$60 bn in early 2001 to c.US$265 bn today driven in large parts by its leading position in the global cancer market (c.30% global market share). Novo Nordisk has been the best performing large-cap pharma stock since 2000, returning a 25% annualised TSR, driven by its dominance of the global insulin market, while the last 20-30 years have seen significant advances in the treatment options of patients, with several diseases including high cholesterol, blood pressure, asthma/ COPD, HIV, cancer etc., becoming manageable chronic conditions. As an example, in the 1990s (pre the introduction of Gleevec, Herceptin, Rituxan etc.) overall survival for patients with various types of cancer was measured in months. Today, if diagnosed early on, these have a limited impact on life expectancy. Admittedly much can still be done for several other cancer types and recent data from immunotherapy agents appear very promising in this regard (see write-up from our US pharma analyst Jami Rubin on the potential for cancer immunotherapy agents). Given the importance of identifying first movers/ability to dominate certain therapeutic areas with high unmet medical needs, we try to identify two therapeutic areas (Alzheimer’s and heart failure) and three technologies (RNAi, cellular-based therapies for cancer/ antibody drug conjugates and oral proteins) which if successful could prove to be happy hunting grounds for risk-friendly investors. Change in number of deaths (between 2000 and 2010) 80% 68% 60% Breast cancer 40% Prostate cancer 20% Heart disease Our broader understanding of the underlying biology behind the incidence of Alzheimer’s disease has improved significantly over the last few years, albeit off a very low base, and on a relative basis is still pretty elementary. This, combined with past failures, means that investor expectations are justifiably low. However, with recent research providing an ability to diagnose patients much earlier on in the disease progression and encouraging data in patients with milder disease we believe there may be some light at the end of the tunnel. If successful, the current late-stage pipeline options could meaningfully change the treatment paradigm for at least a sub-set of the Alzheimer’s patient (by helping slow the progression of the disease as opposed to providing short-term symptomatic relief). There are two approaches being evaluated by three companies in late-stage development – the amyloid-β antibody hypothesis and the β-secretase inhibitors (BACE) hypothesis. On the amyloid-β antibody hypothesis, Eli Lilly (Sell; US$59.4, covered by Jami Rubin) has ongoing Phase III trials evaluating solanezumab (data expected in 2016/17) and Roche (CL Buy, SFr264.5, Keyur Parekh) have two assets in mid-late stage development, gantenerumab (in Phase II/III studies) and crenezumab (Phase II data expected mid2014). Merck & Co (Neutral, US$56.9, Jami Rubin) is evaluating the use of its BACE inhibitor (MK 8931) in a phase III study, which will report data in 2017/18. If successful, Alzheimer’s could be one of the biggest commercial opportunities this industry has ever seen (US$50-100 bn). Number of people with dementia worldwide (2010-50), original (2009) and updated (2013) 140 135 mn 115 mn Population with dementia (millions) Our European Pharma analysts discuss emerging therapeutic areas 105 76 mn 70 66 mn 2013: 44mn 35 33 mn 0 2010 2030 Original Stroke 0% -2% -8% -20% HIV -16% -23% Alzheimer's Disease -40% -42% -60% Source: Alzheimer's Association. Alzheimer’s disease: A disease, who’s total societal cost is estimated (Alzheimer's Disease International) at c.US$600 bn (1% of world GDP), impacting c.44/5 mn patients globally/US (2050E 135/16 mn). In 2013, the direct costs of caring for those with Alzheimer’s in America will total an estimated US$203 bn, including US$142 bn in costs to Medicare/ Medicaid. Net net, the burden of this disease is not only huge, but also increasing and current treatment options (Aricept, Exelon, Razadyne, Cognex, Namenda) are sub-optimal at best. As Alzheimer’s progresses, brain cells die and connections among cells are lost, causing cognitive symptoms to worsen. While current medications cannot stop the damage Alzheimer’s causes to brain cells, they may help lessen or stabilize symptoms for a limited time (6-12 months) by affecting certain chemicals involved in carrying messages among the brain's nerve cells. Goldman Sachs Global Investment Research 2050 Updated Source: Alzheimer's Disease international - The global voice on dementia. Heart failure (HF): Arises when the heart cannot pump enough blood to meet the body’s needs. It is estimated (WHO) that over 23 mn people worldwide suffer from HF and the prevalence rate is expected to increase with an ageing population and rising risks from co-morbidities, such as obesity, hypertension, and coronary artery disease. Despite significant advances in therapeutic options in the past decades, HF remains a life-threatening disease with an annual mortality rate of 10%, on par with many types of cancer, indicating significant unmet medical needs for many patients. The current treatment paradigm for chronic heart failure includes a combination of diuretics, ACE inhibitors, angiotensin-receptor blockers (ARB), mineralocorticoid receptor antagonists (MRAs), and beta-blockers. For acute heart failure, inotropes are also added to enhance the ability of the heart to pump blood. Most of these drugs were approved in 1990s or even earlier, and innovation in this area has been relatively quiet in the past decade. However, with better understanding of the underlying disease, we may have just entered a new era of drug discovery in HF. The market opportunity for new therapies could be US$5-10 bn+ given the relatively high unmet medical needs. 5 Fortnightly Thoughts We highlight several pipeline drugs that may improve the current standard of care in HF: (1) Novartis’ serelaxin, a form of a naturally occurring hormone (human relaxin-2), which helps pregnant women to cope with the additional burden on the cardiovascular system by increasing blood output from the heart and blood flow in the kidney. Data from a late stage clinical trial suggest serelaxin could improve short-term symptoms of acute heart failure patients after hospitalisation, and may also reduce the mortality risk. (2) Novartis’s LCZ696, a first-in-class combination drug of two active ingredients, its block buster drug Diovan and a novel neprilysin inhibitor AHU-377. The drug has the potential to restore the natural neuro-hormonal balance in HF patients. (3) Bayer’s BAY 94-8862, a new generation MRA that offers more specificity and a better safety profile. (4) Amgen’s AMG 423, a novel stimulator of the activity of heart muscle. The drug has shown some signs of clinical benefit in early-stage clinical trials. (5) Stem cell therapies, e.g. MyoCell from Bioheart that uses a patient’s own muscle stem cells to repair heart muscle. The re-birth of RNAi: Our DNA is a collection of genetic recipes to make proteins, which are the makeup of our body. While most proteins are important for our day-to-day function, sometimes the genetic recipes are faulty and become disease-causing proteins. RNA interference (RNAi), also known as gene silencing, is a novel technology where ‘intercept messengers’ are inserted into an organ or tissue and stop disease-causing proteins from being made. Because RNAi targets a specific gene, it is theoretically possible to create a drug that is highly specific to a disease, target any organ, with a low side effect profile. Secondly, the ability for RNAi to enter tissues directly means that it can target a broader range of diseases than the traditional “white pill” and antibody drugs that often can only act on the surface of tissues. There was an early wave of interest in RNAi technology in the late 2000s, with expectations that it would revolutionise drug treatment and reduce the average time it would take to get a drug to market. This was further fuelled by the Nobel Prize award to Andrew Fire and Craig Mello for their discovery of RNAi in 2006. Over the next few years, several major deals/partnerships were forged, including the Merck & Co acquisition of Sirna (US$1.1 bn, 2006), and Roche’s acquisition of Mirus Bio (US$125 mn, 2008). However, several major setbacks (Allergan, Pfizer, Tekmira etc.) beset the first generation of RNAi therapeutics as researchers realised that drug delivery to organs was more complex than initially thought, and some first generation therapeutics showed undesired side effects such as switching off genes that looked similar to the target gene, and undesired activation of the body’s immune system. Given these disappointments, large-cap pharma’s have in most part chosen to exit this area, with both Merck and Roche divesting their originally acquired assets and significantly reducing their R&D efforts in this space. However, more recently, AstraZeneca (AZN) and Sanofi (SNY) have upped their interest in this technology. AZN agreed with Moderna Therapeutics to develop messenger RNA therapeutics in cardiometabolic diseases and cancer, and SNY acquired a US$700 mn stake in Alnylam driven by renewed interest in the new refined RNAi therapeutics. Key players now include Alnylam, ISIS, Opko Health, Santaris Pharma, and Arrowhead Research. These companies have focused their efforts on making RNAi more specific to the target gene, improving the drug delivery systems and reducing the impact to the immune system in the hope that that these treatments can target more difficult to access organs and have a cleaner side effect profile. This allows RNAi therapeutics to be developed for a wider range of diseases, including cancers, viral infection, autoimmune and neurodegenerative diseases. Goldman Sachs Global Investment Research Issue 70 Cancer approaches beyond immunotherapy: In addition to the interesting developments in the cancer immunotherapy field, we believe several other approaches are very exciting opportunities including cellular based therapy (CAR-T) and antibody drug conjugates (ADC) which could change the way we think about cancer treatment. Cellular based therapy for cancer: New advances in cellular based therapies have hinted at a potential breakthrough for some intractable forms of blood cancer. In short, cellular-based therapy for cancer uses the patient’s own T-cells (immune effector cells) to actively target and eradicate their cancer. The process involves harvesting a patient’s own cells and inserting new genes that allow them to home in on cancer cells. Once these modified cells are reintroduced into the patient the body is able to mount an effective immune response against the cancer. While stimulation of the immune system leads to some severe side effects, this therapy has yielded complete and durable remissions in some patients. The technology underlying this cellular therapy is known as CAR-T (chimeric antigen receptor T-cells). Essentially, the technology builds upon the experience of using monoclonal antibodies to specifically target antigens on the surface of cancer cells. This is much like the effect that Rituxan, which specifically targets a cellular marker on B-cells (CD20) to deplete the body of cancerous cells. These antibodies, however, rely on other effector cells to carry out tumour cell killing and are unable to fully mobilise or amplify the body’s immune response. CARs overcome this limitation via the modified T-cells which possess the antibody-like capability of specifically binding to cancer cells, but also bring the direct killing effects of T-cells. These T-cells remain active and can destroy a greater number of cancer cells in addition to having the ability to further amplify the immune response. Several recent studies have indicated dramatic efficacy results, including complete and durable remissions in some patients. The University of Pennsylvania, in collaboration with Novartis recently presented data showing that a large subset of blood cancer patients treated with CAR-T therapy achieved remission. Memorial Sloan Kettering Cancer Center recently reported similar results in its study of modified T-cells in patients with advanced leukaemia. While enrolment was relatively small, 88% of patients achieved a complete response, compared to the 30% chance of achieving a complete response for patients receiving standard chemotherapy. While the initial efficacy benefits of the CAR approach have yielded encouraging results, there are still many technical challenges. First is the management of the often severe and potentially life threatening side effects that come with stimulation of the immune system. Researchers are currently working to create a treatment protocol for these side effects in addition to attempting to predict which patients are likely to suffer from these effects. There are some practical hurdles as well (time to harvest, process and reintroduce, impact of chemotherapy on T-cells etc). To circumvent these hurdles, several start-up companies and research groups have proposed using T-cells from donors that have been further engineered to properly function in transplant recipients. Antibody drug conjugates (ADCs): ADCs are a new class of highly potent biopharmaceutical drugs designed as a targeted therapy for the treatment cancer. ADCs are complex molecules composed of an antibody linked via a stable, chemical, linker with labile bonds, to a biological active cytotoxic (anticancer) payload or drug. By combining the unique targeting capabilities of monoclonal antibodies with the cancer-killing ability of cytotoxic drugs, antibodydrug conjugates allow sensitive discrimination between healthy and diseased tissue. This means that, in contrast to traditional chemotherapeutic agents, antibody-drug conjugates target and attack the cancer cell so that healthy cells are less severely 6 Fortnightly Thoughts affected. We believe Roche and Seattle Genetics are leading the field on ADC’s with >20 programmes currently in clinical and preclinical development across multiple tumour types. Oral Proteins/ peptides: Historically, oral dosing of proteins has been an enigma, with several failed attempts thus far. However, two recent events have reignited interest in this field with Novo Nordisk attempting an oral version of its injectable GLP-1 drug (semaglutide), with positive early stage data leading to Novo initiating a phase II study (data expected 2015). While clinically very exciting, the commercial uptake of the GLP-1 class in treatment of type II diabetes has been hindered in part by their injectable route of administration and consequently, we believe that if it was possible to create an oral version of GLP-1, it could lead to significantly higher penetration and greater market share (5x-10x the current GLP-1 penetration). In a similar vein, Roche has announced its decision to in-license an oral version of octreotide acetate (a peptide) from Chiasma (based on its proprietary TPE™ System, TPE is an acronym for "Transient Permeability Enhancer"). The TPE enables oral delivery of macromolecules (up to 20 kDa in size) and poorly-absorbed small molecules through the intestine wall into the systemic circulation. Goldman Sachs Global Investment Research Issue 70 With the use of the TPE System certain currently available injectable drugs could be switched to oral formulations and potentially expanding the market for these drugs. Octreotide is currently sold for use in several diseases including acromegly and some neuro-endocrine tumours. While certainly not for the faint hearted, we believe the above therapeutic/ technology break-through could provide meaningfully outsized returns if successful. Change is indeed a constant, but identifying it early could lead to meaningful investing opportunities. Keyur Parekh / Steve Chesney / Eleanor Fung / Mick Readey European Pharma analysts email: Tel: [email protected] / [email protected] / [email protected] / [email protected] Goldman Sachs International +44-20-7552-9939 / +44-20-7552-9371 / +44-20-7774-6518/ +44-207552-3714 7 Fortnightly Thoughts Issue 70 Interview with...Sir John Chisholm Sir John Chisholm is the Executive Chairman of Genomics England, a company set up by the Department of Health in the UK to deliver the ‘100,000 Genome Project’ under which 100,000 whole genomes from patients with genomically important diseases will be sequenced over the next four years. He also serves as the Chair of Nesta, an independent charity that promotes innovation in the UK and has previously served as the Chairman of QinetiQ Group. Hugo Scott-Gall: What is genomics and what does it mean for healthcare? Sir John Chisholm: Let’s start with the genome. A human genome consists of about 3.3 billion base pairs of DNA which together code everything that human cells do. And so, it was thought that when a human genome is decoded, a fantastic cornucopia of insights would emerge. That gave birth to the Human Genome Project which sequenced a human genome for the first time at the turn of the century at a total cost of about US$3 bn. But biological processes which make us what we are today, having evolved with the earth for over 4 bn years, turned out to be fearsomely complex and difficult to analyse. Instances where a single gene codes for a specific syndrome were found to be relatively few, with the vast majority of human syndromes actually involving simultaneous activities of multiple genes. Furthermore, contrary to previous belief that proteins were perhaps the most important in cell biology, given that they are the molecular vehicles which dictate how disease paths work, it was realized that the regulation of protein formation is at least as important as the proteins themselves. Since then, through progressive improvements in sequencing capabilities, we have moved from the first-generation sequences of the Human Genome Project to much more advanced secondgeneration sequencers that we deal with today. Consequently, the cost of sequencing has fallen dramatically at a pace even faster than Moore’s law suggests. With the sequencing cost of a whole human genome reaching below £5,000 in 2012, it became feasible to conceive of a large-scale sequencing project and this is when we kicked off the ‘100,000 Genome Project’ in the UK. The Prime Minister launched it at the end of 2012 and Genomics England got going by mid-2013. Given the complexity of how genes work together, correlating them with specific phenotypes requires a study of a large sample number of patients to successfully identify combinations and unique characteristics. Our project, with a goal of 100,000 genomes, is two orders of magnitude more than any single collection that's been attempted thus far. It is a very bold step which can radically change the way medicine is practiced. Today, diagnosis relies on the expertise of the individual clinicians, but this project will help healthcare transform, putting highly analytical, data-driven information in the hands of clinicians so that the treatments that patients get are based on a much more precise diagnosis that stems from an acute understanding of the condition that they are afflicted with. It’s difficult to say precisely how long it will take to develop the datadriven industry that will be able to deliver this, but as healthcare steadily becomes more data-driven, different skills will be required from participants in the healthcare chain compared to what has been the case historically. Goldman Sachs Global Investment Research Also, if treatments can be prescribed for the precise syndrome of an individual, the opportunity for a single global mega-drug which does almost everything is reduced. And so, it is likely that many more specific molecules will be developed, each of which may have a much smaller market of their own. It’s also possible to imagine a situation in the future in which a precise molecule may be designed through some automatic process, based on the molecular diagnosis of a patient. While that's science fiction at the moment, it is the direction in which the industry is headed. It’s also possible to imagine a situation in the future in which a precise molecule may be designed through some automatic process, based on the molecular diagnosis of a patient. While that's science fiction at the moment, it is the direction in which the industry is headed. Hugo Scott-Gall: What are the big gating factors and challenges that you face in your field? Sir John Chisholm: What we are doing is still pretty much at the edge of science. The phenomenal complexity of the biological systems and the technological difficulties of sequencing certainly pose a significant challenge. But, while the sequencing machines are not yet perfect, they will definitely get better as we progress in the project. However, an even bigger challenge is that even after getting a genome that is 99.5% or 99.9% accurate and linking it to the clinical phenotypic data of the patient, translating and decoding the data into actionable treatments for individual patients is still at or even beyond the edge of science at the moment. To give you some context, of the three million variants that all of us have from a standard genome, we typically understand only 15,000 as of now. This is why projects like ours are important steps through which we will steadily discover the remaining unexplored regions of this science. Hugo Scott-Gall: The benefits of this will be tremendous... Sir John Chisholm: Absolutely. Some people estimate, for example, that just 30% of cancer treatments offered currently are actually relevant to the precise presentation of an individual’s cancer. And we now know that every cancer is different. There is a huge loss of efficiency which the molecular diagnosis treatment can help overcome by providing an exact understanding of the mutations that causes the cancer in the body. Once the disease is understood that precisely, doctors will be able to go through the list of non-toxic molecules available and choose the one which has the right characteristics to deal with that particular mutation. This opens up a new set of possibilities because we may find that certain products may be relevant for syndromes for which they were previously never considered appropriate. Going down this route will make it possible, for instance, to treat a patient suffering from ovarian 8 Fortnightly Thoughts cancer with a molecule that has actually been developed for breast cancer. Hugo Scott-Gall: Will the benefits apply to rare diseases as well? Sir John Chisholm: The impact on the treatment of cancer and rare diseases will be slightly different. As we sequence more wholegenomes of cancer patients, it is likely that each variation of cancer will become a small sub-type of the disease. So, instead of just knowing that they have melanoma, people will be able to identify that they have melanoma with BRAF v600e mutation, for example, and get a different treatment appropriately. For rare diseases, we will be able to define the disease itself better. Instead of thinking of it as a general developmental disorder which is very difficult to treat, if we are able to identify the precise genetic cause of the problem, we will be able to target it better through specific gene therapy or some sort of protein replacement. The health economics of treating rare diseases is very attractive, particularly if the patient is young and with a huge part of their productive life ahead of him or her. Rare Mendelian diseases, i.e., diseases caused by inherited mutations of the genome, have mostly proved in the past to be extremely difficult to deal with. What decoding the genome gives us the opportunity to do is to conceive of ways in which you might be able to treat rare diseases which are today totally untreatable. How society deals with the fact that it will be possible to discover mutations in individuals that predict future healthcare expenses will be an important ethical question and is definitely an issue for society to grapple with. But that is a consequence of being able to discover such diseases now and having the possibilities of dealing with these. Hugo Scott-Gall: Which countries are making the most progress in the field? Also, is the world joined up in its efforts to develop genomics further? Sir John Chisholm: There are a lot of global joined-up endeavours in which the scientific community is seeking to learn from each other and is working towards common standards so that the tools which are being developed in one place can readily be adopted elsewhere. So at one level, the world is quite well joined up. However, in order to make a widespread adoption of genomics practical, genomicists need to operate with national health systems which tend to be rather more idiosyncratic, and in most cases, highly fragmented. In this context, the UK is particularly well placed to take a lead in this technology, not only because we have developed a very strong scientific understanding of genomics and its clinical consequences, but also because we have an integrated single payer health system. These two things don't co-exist anywhere else in the world at the scale we have, and this was the key reason why David Cameron could push for the UK to become a leader in this field. For instance, unlike the UK, the US doesn’t have just one payer that can decide to generate the samples and the data that is required to feed a project like ours. Being an insurance-based health system which is very fragmented, getting together a patient community of the size and characteristics that are required for a programme like ours becomes very difficult to do in the US. The Goldman Sachs Global Investment Research Issue 70 same is true for China which is reflected in the fact that they have only been able to sequence 15,000 whole genomes thus far. So, while some other smaller countries, a number of which are in the Persian Gulf, have recently announced similar projects, there might be considerable work to be done in drawing appropriate data from their health system. Hugo Scott-Gall: How will the privacy risks be addressed with regard to the data that will be collected for this project? Sir John Chisholm: We ensure two things are true in order to manage such risks in our project. First, our project is based on the consent of all the participants. We explain to all patients exactly what we are going to do with the samples and data they provide and how it will be the subject of considerable research by many academic, clinical and industrial bodies. We also clarify that the outcome may not benefit them specifically but instead form a key part of the large dataset from which insights will be gathered, that together are likely to benefit the broad patient community. So, only patients providing us with an informed consent form a part of this project. Secondly, we commit to the anonymization of the data so that nothing can be traced back to an individual easily. All the collected data is retained within a National Health Service firewall so that only those people who have satisfied us that their enquiries are legitimate will be let behind the firewall to do specific studies and have access to the data. Users will be able to pay for access to the anonymized dataset but will not be able to take the data away with them. Hugo Scott-Gall: From a broader point of view, what role can governments play in sparking and fostering innovation, particularly in fields that require a significant amount of risk capital with very long-term paybacks? Sir John Chisholm: Governments certainly have a big role to play. In fact, many of the most radical economic changes in the last 300 years or so have been driven initially by non-economic actors – be it philanthropy, governments or asset bubbles. In order to get a profoundly new technology into the market, the first investors are very unlikely to generate significant returns. Take the rail networks or the internet, for example. While those that founded them did not make a lot of money themselves, they provided an infrastructure from which huge wealth was ultimately generated. And investing in profoundly new infrastructure like these is indeed one of the key roles of the government. It's impossible to know at the outset what products and services will ultimately come from such an innovation, but, by providing that infrastructure, governments can give the market economy an opportunity to exploit it. That is what is happening with genomics too; we're providing an infrastructure which is our data set. We can't predict exactly what products and services will emerge from it and when, but we know for sure that once mined, the tremendous data that a genome holds about biological activity will profoundly affect humanity. It's a very smart idea for a country to be the first to generate an economic space for the market to exploit. 9 Fortnightly Thoughts Issue 70 Genomics: Changing pharma Isaac Ro, our US Life Sciences analyst, seeks the potential in genomics The cost of sequencing a human genome has declined at an extraordinary pace over the last seven years, more than 1,000-fold thanks to the advent of next-generation DNA sequencing (NGS). An experiment that was once a multi-year process requiring hundreds of dedicated scientists, dozens of instruments, and millions of dollars in funding can now be done by a single person in just days with a variable cost of US$1,000 using Illumina's (ILMN) latest technology. This type of performance breakthrough has shattered the famous Moore's Law in semiconductors and ushered in a new era of scientific discovery. 50k human genomes had been sequenced cumulatively by the end of 2013. Looking forward, just one of ILMN's HiSeq X Ten installations will be capable of generating 18k genomes per year. We expect volumes to be driven by large research labs (i.e.: The Broad Institute at Harvard/MIT), drug companies (REGN, AMGN have both announced plans), and new commercial research labs (i.e.: Human Longevity Inc, a privately held commercial lab headed by Craig Venter). The Broad Institute expects to more than triple output in 2014 Data output measured by number of terabases 2,500 2,064 2,000 Rather than looking at highly isolated portions of the genetic code (usually a fraction of 1%), scientists can now look at a person's entire genome in a snapshot and do so repeatedly over time as mutations occur and change. ILMN's dramatically less expensive/ faster technology thus enables scientists to take a true "open hypothesis" based approach to genetics, rather than aiming for "hot spots" in the genome and hoping to find key mutations. A practical analogy: if you drop a coin in the dark, you are more apt to find it using a floodlight than a flashlight. With this in mind, we consider the potential for NGS to power a wave of disruption in the pharmaceutical industry by redefining the way in which patients are matched with drugs. Did you know that...? The first human genome took 13 years and about US$1 bn to sequence? Today, it takes days at a cost closer to US$1,000 Pharma: A near term beneficiary of NGS Near term, we anticipate the pharma industry, primarily in the field of cancer, to be the greatest beneficiary of the democratization and explosion of genomic data. A growing body of work has illustrated that cancer is a disease that must be identified and treated according to its genetic underpinnings, which can only be elucidated using NGS. Cancer has historically been characterized by its tissue of origin (lung, breast, prostate) but the scientific literature increasingly shows that many cancers are better defined by the genetic pathways or mutations that cause them. In reality, the tissue of origin for a given cancer is often the by-product, not the cause, of disease. At the same time, a significant percentage of first line cancer therapies are ineffective and carry adverse side effects. By using NGS, physicians can identify the genetic signature of a patient's cancer and use that information to make more precise treatment decisions. This has the combined benefit of improving patient outcomes while also reducing the use of drugs that are known to be ineffective against certain mutations. The implications here could be massive, both for biopharma R&D programmes (where NGS can improve the likelihood of success in the drug development process) and for payers (where significant amounts of wasteful spending on ineffective drugs can be reduced). That said, we believe that NGS still faces two key bottlenecks before it can take its place as an everyday tool in modern medicine: bioinformatics and regulation. Bioinformatics and Big Data; a potential bottleneck We anticipate explosive growth in the amount of genomic data that will be generated over the next few years. For reference, less than Goldman Sachs Global Investment Research 1,500 1,000 660 500 303 362 154 23 0 2009 2010 2011 2012 2013 2014e Source: The Broad Institute. At the same time, the data generated by NGS is huge and lacks standards. Today, an average human genome file is 65GB in size. In addition, no software standards yet exist to define what constitutes a properly formatted and high quality human genome. In fact, the vast majority of NGS software tools used today have been developed in academic labs as "homebrew" solutions which we do not believe will scale over time as commercial products. That said, NGS is here to stay and Pandora's Box has already been opened in the clinical setting. As a result, we see a rapidly emerging need for highly scalable interpretive bioinformatics tools. As these tools emerge, we see a rapidly emerging shift in the NGS value chain toward software to help process the vast amounts of data that could pose a simultaneous threat and opportunity to current stakeholders. The good news is that all of the key players recognize the need for industry standards. Companies including Illumina, Google, Merck & Co, and the New York Genome Center have partnered in the Global Alliance for Genomics and Health – an organization dedicated to standards, policies, and technology to improve human health. We believe that alliances and efforts such as these are likely to result in the formation of genomic industry standards. In the meantime, a lack of standards has led pharma companies to become creative in obtaining relevant genomics data to accelerate the discovery and development of novel therapeutics (chiefly in the field of oncology). Partnerships with research labs and clinical diagnostics companies such as Foundation Medicine (FMI) have been the primary avenues that pharma has taken to date, although we see the potential for in-house labs to rapidly emerge as well. For example, Regeneron (REGN) has partnered with Geisinger Health in a major human genetics research collaboration, where the two plan to sequence samples from more than 100,000 patients. Amgen has taken the in-house approach through its acquisition of deCODE Genetics. AMGN will utilise deCODE’s previous database as well as continue sequencing studies in-house. We believe that partnerships will create a positive feedback loop for both the academic centres and clinical diagnostics companies as their databases grow, making them more valuable to both current 10 Fortnightly Thoughts and future pharma customers. This raises the second key issue as NGS expands into the clinical setting: who owns the data and how will this technology be regulated? Issue 70 FMI has partnered with numerous pharma companies Press released partnerships between FMI and pharma companies The regulatory landscape is a work in progress Company Name Ticker Target Announce Date The second major hurdle to broader clinical adoption of NGS is an uncertain regulatory landscape. While the FDA has approved ILMN’s MiSeqDx instrument for clinical use, it has fallen to providers of clinical diagnostic tests to choose whether or not to obtain FDA approval for these diagnostic tests or choose the less regulated “CLIA waived” lab-developed-test path (not regulated by the FDA). Agios Pharma AGIO IDH1 or IDH2 enxymes (cancer metabolism) Apr 4, 2013 ARIAD Pharma ARIA ALK/EGFR inhibitor for NSCLC Nov 13, 2012 Array BioPharma ARRY Drug treatments Mar 6, 2012 AZN (London) Genomic predictors of response to drugs Nov 12, 2012 CELG Not specified/various May 17, 2011 CLVS PARP inhibitors Aug 6, 2012 4523 (Tokyo) Clinical trials and drug development Oct 9, 2012 N/A (Private) Lung Cancer November 7, 2013 JNJ Oncology clinical development Oct 25, 2011 Memorial Sloan-Kettering N/A (Private) Hematologic cancers May 2, 2013 Novartis NOVN (Zurich) Not specified/various Jan 4, 2011 - Jun 7, 2012 Jan 6, 2014 Sanofi SAN (Paris) Biomarkers for drug candidates Jan 10, 2012 While this pathway has served as a suitable solution for sequencing providers offering genetic testing solutions in the field of reproductive health and oncology, questions have emerged regarding the nascent but growing field of companion diagnostics (CDx) based on NGS. For background, CDx are tests are used in concert with pharmaceuticals to better align patients with associated therapies. Today the market for CDx is comprised primarily of first generation offerings targeting specific mutations in specific genes (KRAS and BRAF mutations for Erbitux and Zelboraf, and ALK mutations for Xalkori). However, we believe that over time the market will shift to CDx offerings that utilise NGS to elucidate a myriad of mutations across multiple gene pathways. The FDA has yet to clearly define a regulatory pathway for companion diagnostic tests and associated therapies. Importantly, lab-developed tests (LDTs) currently present a secondary pathway by which tests can be developed, and these remain potential competitors to the official companion diagnostic that is co-developed with the pharmaceutical company. This potential competition creates a disincentive for diagnostic companies to invest. This lack of clarity subsequently clouds the willingness of insurance companies to pay for these tests as well. Current billing practices do not allow payers to discriminate between an LDT and an FDAlabelled CDx. Thus, diagnostic companies that invest in a companion diagnostic programme may not ultimately see the rewards. Finally, these new methods of drug development are based on genetic pathways, while FDA labelling is based on disease or tumor location. Thus, ongoing research increasingly identifies potential drug uses that are not covered by the official FDA label. We highlight FMI’s ability to match drugs to specific genetic mutations in tumor cells as evidence of this growing trend. When this occurs, physicians are often forced to resort to off-label use given the typically limited lifespan of patients. As scientific advancements accelerate faster than regulatory pathways, we expect that payers will be increasingly forced to decide whether or not to reimburse off-label drug use. Goldman Sachs Global Investment Research AstraZeneca Celgene Clovis Oncology Eisai Friends of Cancer Research and others J&J Source: Company data. Despite headwinds, long-term outlook is exceedingly positive Despite these headwinds, we expect NGS technologies to continue to proliferate in clinical use. Nearly every late-stage cancer therapeutic today is being developed in conjunction with a companion test. We expect the interface between pharma companies and research labs, both private and public, to expand significantly in the near term. These partnerships should result in increasingly large genomic databases, which would help expand the trend of targeted therapies into other therapeutic areas beyond cancer. Regarding pharmaceutical companies, we expect blockbuster first-line therapies to become increasingly rare. Targeted therapies and companion diagnostics generally serve to limit the TAM of new drugs, but will likely help to accelerate adoption given improved efficacy. Whatever the exact financial consequences, it is clear that development of the next generation of drugs will require strong integration with NGS technologies Isaac Ro US Life Science Tools & Diagnostics analyst email: Tel: [email protected] +1-212-902-6393 Goldman, Sachs & Co. 11 Fortnightly Thoughts Issue 70 Interview with... Dr. Peter Bach Dr. Peter Bach is the Director for Health Policy and Outcomes at Memorial Sloan-Kettering Cancer Center. His research focuses on healthcare policy, in particular cancer payment, developing models of alternative reimbursement and coverage policies. He serves on several national committees and The World Economic Forum’s Global Agenda Council on Health Technology. Hugo Scott-Gall: How do you look at the progress that has been made in the treatment of cancer? Peter Bach: Only the most cynical could discount the meaningful progress we're making in therapeutics in cancer. We have not cured cancer, but we are very, very slowly driving down the mortality rate. The Human Genome Project has led to an understanding of the mechanisms of disease leading to the identification of what we call driver mutations and the understandings of those mechanisms, and then agents that block those mutations and/or their activities and we can clearly see substantively better outcomes for patients. I believe this will serve to accelerate the number of identified types of mutations and mechanisms from where we are today , at about a half dozen linked to approved drugs, to twenty or more in the next three years. So, that's a positive trend and progress that matters. Hugo Scott-Gall: But this progress comes at a steadily rising price... Peter Bach: Right. These advances have been accompanied by a consistent rise in the pricing of therapeutics in oncology. Prices have risen so rapidly that it is difficult to determine what they are correlated to. Currently, the justification given as the most important determinant of pricing for a new cancer drug is the price at which the previous drug came onto the market, and not how well the new drug works or how innovative it is. In the past few years, this pricing trend has spilled over into other specialty diseases such as rheumatoid arthritis, multiple sclerosis, cystic fibrosis and Hepatitis C where drug pricing isn’t linked to any reproducible or predictable notion of value either. So the lack of price discrimination based on any metric of value, whether crude or highly specific, is a substantive problem. This has had implications for health insurance. As the insurance industry has to increasingly manage high-priced drugs, while also trying to create more affordable insurance products, the result is that more of the costs are put on the patient. So we see not only rising premiums, but also rising co-insurance and co-payments. This is a worrisome trend, particularly on the patient out of pocket side. Our system fails when we make scientific progress but then patients cannot afford to avail themselves of that progress because they are priced out. For example, the generic drug for breast cancer Tamoxifen, which has saved more lives from cancer deaths than most other drugs, has a co-payment attached to it in most plans. This makes no sense. Studies show women have stopped taking their Tamoxifen because of the out of pocket costs. Meanwhile, no woman would overuse the drug because of its side effects, so the whole idea of using co-payments to give patients ‘skin in the game’ has no role here or with any therapy we have that is substantially net beneficial. We can fret about the cost to taxpayers, the financial burden and indebtedness for future generations and our economic lack of competitiveness. But the worst manifestation is that whether it is Goldman Sachs Global Investment Research tamoxifen or a new expensive drug, if it actually works, or is less toxic, that's something that took huge investment of dollars, time, and the good will of research participants, and it shouldn’t be squandered due to poorly designed insurance products. Hugo Scott-Gall: How can this pricing dynamic change in the US? Peter Bach: A quote often attributed to Winston Churchill comes to mind: "Americans will always do the right thing... but only after they have exhausted all other possibilities." There are a number of other possibilities still left on the table, and it will take a while to work through them. But I foresee one of two scenarios being ultimately viable. A drug that really adds value would therefore naturally garner two things in the marketplace; a monopoly price and a universal patient base. First, I believe we should tie the price of healthcare to its value. If done correctly, this would reward the producers of value, the successful pharma companies too, because the drug would be offered as a core piece of the insurance product. A drug that really adds value would therefore naturally garner two things in the marketplace; a monopoly price and a universal patient base. Insurance would also work in the way it's supposed to - people don’t have to pay out of pocket to get access to important treatments. The rationale is similar to car insurance in the US, where there is zero cost glass coverage, as it is not desirable to have people driving around with broken windshields, and also because most glass isn't broken as a result of anyone's fault. So, in a value-based system, we would pay for drugs according to their incremental value, but what that calculation looks like is something no one is even close to figuring out. To be specific, we could probably figure out what goes into the formula, but we are far from assigning the coefficients. Then the flip side is me-too drugs, drugs that are only marginally or no more beneficial than something else we already have. They wouldn't be able to get a premium price, which is what happens today. In fact, we would work very hard to get them to compete with their me-too counterparts to drive down the price of both. That’s the way markets are supposed to work. This will happen in the future. But what I believe is more likely to occur today will grow out of our putting more risk on providers. The buzz-word surrounding this trend in healthcare is “risk sharing” or “risk shifting”. The idea, very much enabled by the Affordable Care Act, is that providers - let's say cancer providers (hospitals, doctors), know more about making the tough choices when treating cancer than anybody else in the system. Therefore, the insurer offers a fixed amount to the provider to treat the patient and go out and purchase the required equipment and medicine. The provider keeps the remainder, which could be the total profit (full risk shift), a certain portion of the total (buffered risk shift) or even a portion of 12 Fortnightly Thoughts what was saved (gain share). There are of course numerous subtle variations, but they all include the same logic that incentivizes the provider to save on costs. An obvious drawback to this risk-sharing scenario is that the strong economic incentives to lower costs may drive doctors to respond more robustly than hoped and the lack of transparency in the system makes it impossible to see what treatment patients are actually receiving. Treatment protocols are usually considered proprietary when they are institutionalized, and certainly when they embedded in service contracts with insurance companies of intermediaries like ‘pathway’ companies. So as someone who is concerned that incentives could lower the quality of care, I find not being able to see what treatment approaches are being standardized worrisome. To avoid a degradation in care quality, we should be able to see what treatment protocols the doctors have agreed to follow and see if those are the best protocols we have for patients with cancer, because if they are not, then we've failed I think our first criterion, which is making sure patients get the best scientifically based treatment we have available. Hugo Scott-Gall: What are the political obstacles to implementing a value-based pricing model in the US? Peter Bach: If this question was posed to me three years ago I would have said pursuing a value-based model is unimaginable in the US. Even today, there is absolutely no way this can be done from Capitol Hill without complete buy-in from the industry. I think the mechanics of it will be difficult, but I think there's been so much pressure on the industry in recent times that pharmaceutical companies are going to start working through something. Historically, the industry has argued that higher prices have to be charged to compensate for the risks taken and to recoup the cost of innovation. However, the industry is now facing pressure from its extremely high prices and more and more questions regarding whether their developments are incrementally valuable or truly meet the unmet needs they claim they do. I do think that there are signs that change is happening. There are a small number of examples here. For example, in an op-ed written in the New York Times, we argued that the price of the cancer drug Zaltrap, developed by Sanofi, relative to a significantly cheaper peer was too high. That resulted in the halving of the price Zaltrap. I wasn't surprised that the New York Times ran the op-ed, but I was flabbergasted that Sanofi lowered its price. It showed that the whole issue of price is a real source of vulnerability for the industry. Moreover, the company’s defense of their price was not that they had created something innovative or better, but rather that they had gauged their price against what the ambient pricing was in the cancer drug space. That argument is a lot less compelling, and in the end it’s tautological too. When Sanofi halved their price overnight, it sent a signal that a lot of companies could do the same if prodded. Hugo Scott-Gall: Does Big Data and technology help with transparency? Peter Bach: A few years ago I would have said no, not really, as Big Data was essentially little data on steroids. However, Big Data seems to be proving out, as it provides sample size for Goldman Sachs Global Investment Research Issue 70 understanding provider level outcomes, which means some day competition between and payment to providers could be anchored to outcomes. Within the data arena, the move towards workable natural language processing is the most exciting. If we can actually render real information from free text, that changes everything. We’ve been working with IBM on Watson, and you can see it working, and that really is a different model. So I predict that in the near future we will see emerging models of reimbursement indices linked to the actual quality of the provider. If so, that does an end to a lot of the transparency challenges we face right now. Hugo Scott-Gall: What role does genomics play in all this? Peter Bach: At the population level, I think the interesting thing is what are the interventions going to be? Identifying a subgroup of individuals who are at risk of cardiovascular disease and monitoring their blood pressure to keep cholesterol down and ask them not to smoke isn’t very valuable. Weren’t they always supposed to do that? Genomic assessment of cancers is a different story, as that is already driving therapeutic decision making and targeted drug development. Hugo Scott-Gall: Could you share your thoughts on advances that may be disruptive to existing treatments? Peter Bach: I'm very excited about immunotherapy, which looks to treat cancer by activating, in one way or another, a component of the patient’s immune system. I’m not alone, immunotherapy was voted “Breakthrough of the year” by Science journal. There’s a long-running joke that cancer vaccines are the future of cancer treatment and always will be...we are going to have to change that joke! Likewise, there is a revolution around understanding the drivers of mutations and creating mechanisms for targeted therapies. If you look at the compounds that have been approved by the FDA and the ones that are in the early phase trials, I do think that the revolution around understanding driver mutations and taking those to mechanisms of action and targeted therapies is going to mean a lot. However, targeted treatments and immunotherapies are not cheap. I think Yervoy is around US$120,000 for a Medicare patient, which is not affordable by any means. If our understanding of mechanisms of disease continues to increase, we may see a material change in development timelines and the historical paradigm of new drugs taking 15 years to develop, with multiple failures along the way could change. This means that that the cost of innovation should come down, and then we should see prices fall and competition increase. Take the Philadelphia chromosome for instance. It was discovered in the 1960s, but the first marketed drug based on the mutation, called Gleevec, was only launched in 2001. That’s 40 years to produce a solution. But things are changing rapidly. Crizotinib, which targets the ALK fusion gene, was only in development for three years before coming to the market, which was about six years after the gene was discovered. If this shrinking of timelines continues it will really be a very exciting and clinically complex time for cancer treatment. 13 Fortnightly Thoughts Issue 70 Cancer immunotherapy is paradigm changing Cancer immunotherapy is paradigm-changing Cancer immunotherapy is potentially the next big wave of anticancer agents. Given the promise for this exciting new class of drugs to affect the survival curve, it will likely “disrupt” the way this insidious disease has been treated. Implications are far reaching with respect to the treatment paradigm, how these drugs are priced and paid for, and which therapies and cancer services could be rendered obsolete (chemo? radiation therapy?). Cancer immunotherapy has become the dominant story in large cap pharma with BMY, MRK and Roche (covered by Keyur Parekh) in the lead, and with numerous trials in late-stage clinical testing. Harnessing the immune system to fight off cancer cells, rather than targeting cancer cells, represents a new approach to treating cancer, and has led to spectacular results. Interest in PD-1/PD-L1 and combination therapies with Yervoy captured the spotlight at ASCO in June 2013, and we expect data to continue to dazzle at this year’s ASCO in June 2014. Initial responses and survival data in some of the most intractable cancers have been impressive, with the potential for a benefit across multiple tumor types. Importantly, these agents have demonstrated the potential for a cure in a subgroup of patients. Approximately 20% of patients on Yervoy (the first immunotherapy checkpoint drug to be introduced to the market) for approximately 10 years have been reported to be alive, which is extraordinary given the high rates of death for late-stage melanoma. Our projections of US$10-15 bn for lung, renal and melanoma looks to be conservative with potential uses across multiple tumor types (hematological, colorectal, head and neck, glioblastoma, etc.), which could support sales of around US$30 bn. so that it can attack and kill cancer cells. They are not directly targeting the cancer cells, but instead are “re-training” the immune system to kill the cancer cells, potentially providing an immune memory and durable effect that leads to a sustained response. This is likely the reason for the impressive durability of responses reported for a broad range of cancers and the observation that patients treated with these drugs experience tumor shrinkage (or tumors not reappearing) even after drug treatment has ended. There are different types of immunotherapy agents, including cytokines (IL-2 and IFN-alpha), cancer vaccines (these are not preventatives, but function to generate an immune response against cancer cells), adoptive T Cell therapy, and checkpoint inhibitors (Yervoy, PD-1, PD-L1). The checkpoint inhibitors have been the main focus of the medical and investor communities, with recent clinical data showing impressive tumor responses, including the potential for a cure in a subset of patient. PD-1 inhibitors are also close to reaching the market, with MRK’s MK-3475 and BMY’s nivolumab both likely to be FDA approved in late 2014 for metastatic melanoma and lung cancer, respectively. Schematic, overall survival curve for single and combo immunooncology drugs Illustrative, not representative of actual data 100 90 80 combo (nivo + Yervoy) 70 Percent Alive Jami Rubin, our US Pharma analyst, delves into the revolutionary potential of immunotherapy 60 nivo 50 40 Yervoy 30 20 10 Immunotherapy can lead to increased long-term survival for a subset of patients vs. chemotherapy and targeted therapies that lead to rapid, but shorter-term survival benefit Illustrative, not representative of actual data Source: Ribas A et al, Clin Cancer Res; 18(2) Jan 2012 Immunotherapy agents work differently from traditional chemotherapy or targeted therapy agents in that it treats the patient as opposed to the specific tumor. Traditional chemotherapy agents function by poisoning and killing cancer cells, but in doing so, also destroys normal healthy cells. Targeted therapies (Avastin, Rituxan, Zelboraf) block/activate mechanisms within the tumor cell so that it can no longer by-pass cell death. As a result, targeted therapies can often selectively kill cancer cells over normal healthy cells. While this is typically less toxic, cancer cells can often build up resistance to these agents. Immunotherapy agents function completely differently. Instead of targeting the cancer cells, they stimulate, enhance and/or restore a patient’s own immune system Goldman Sachs Global Investment Research 0 0 0.5 1 1.5 2 2.5 3 3.5 4 Years Source: ASCO 2013: Walter John Urba, MD, PhD. Yervoy targets CTLA4, an immune checkpoint that dampens the body’s immune response early in the activation cascade by inhibiting T-helper cells (activates immune response) and stimulating regulatory T-cells (suppresses immune response). By blocking CTLA4, Yervoy broadly enhances the immune response and boosts the body’s natural ability to attack tumors, particularly those that are immunogenic, like metastatic melanoma. However, excessive immune system activity can cause significant side effects, such as GI and skin toxicities (e.g. colitis and dermatitis) although they can be managed with careful dosing and corticosteroids. Yervoy became the first checkpoint immunotherapy agent approved for metastatic melanoma in 2011 and has been shown to improve survival. PD-1/PD-L1, like BMY’s nivolumab and MRK’s MK-3475, have generated the most amount of excitement because unlike CTLA4 which acts upstream in immune activation, PD-1 dampens activity later in the immune cascade at the time and site of the inflammatory response, and have shown better responses and less toxicities than Yervoy. The PD-1 receptor is present more broadly than CTLA4 and can be found on T-cells, B-cells, and NK cells, among others. There are multiple additional pathways that can be exploited for cancer immunotherapy. Currently BMY’s leading portfolio includes a LAG3 antibody, lirilumab (anti-KIR, which is partnered with Innate Pharma, covered by Steve Chesney), Urelumab (anti-CD137) and denenicokin (interleukin 21). 14 Fortnightly Thoughts Issue 70 Data to date looks impressive Initial data from cancer immunotherapy drugs, i.e., checkpoint inhibitors, has been impressive. Initial responses for Yervoy were mid-single digits to mid-teens, but even more notable is that for certain patients Yervoy represents a potential cure (10 year survival rates are 20%). Initial data from BMY’s Nivo, MRK’s MK-3475 and Roche’s PD-L1 have already shown response rates higher than that seen with Yervoy. Response rates across lung, melanoma and renal have been encouraging. And initial overall survival data for Nivo improved upon the results seen with Yervoy. Nivo had a 43% 2-year survival in advanced melanoma compared to Yervoy data of 25%-30%. We have also seen strong, long-term survival rates in NSCLC and RCC with Nivo. The lasted data in squamous and nonsquamous NSCLC demonstrated a 1 year survival of 42% and 2 year survival of 24% in patients treated across all doses. We could potentially see even higher OR rates with the best dose (3 mg) which is currently in Phase 3 studies. Sizing the commercial market The cancer market is expected to be around US$80 bn in the developed markets and close to US$20 bn in the pharma-emerging markets, according to IMS. We believe that the market’s understanding of the size of the immuno-oncology market is still early in its formation. Our GS pharma team has published an initial estimate of US$10-15 bn, but this is likely too conservative as it only includes revenues for lung, renal and melanoma. There is clearly upside to our forecast from the numerous other tumor types that are being explored. BMY is currently exploring around 10 tumor types for Nivo, including lung, renal, melanoma, gliobastoma, triple negative breast, gastric, pancreatic, prostate cancer, hematological cancers, and hepatocellular cancers. chemotherapy agents are used today; as a first line treatment across a diverse range of tumors. If that becomes the case it will put clear pressure on the sales of some of the current treatment regimens. Target therapies/chemotherapies such as LLY/Alimta and ROG/Avastin (used for lung as well as other cancers) may lose out. Companies and investors are watching as immuno-oncology agents progress in additional cancer types as their usage may be wide-spread, disrupting many current cancer drugs and/or targeted therapies in pharma/biotech pipelines. While there is potential for combination targeted therapy with a PD-1 antibody, we have yet to see any clinical data on this, though ROG has started a combination PDL-1/Avastin study as has BMY. Those companies that have access to PD-1 molecules, will clearly be advantaged in a world where immuno-onocolgy is the backbone of cancer treatment. Biomarkers One area of debate in the field remains around the need for PD-L1 biomarkers. There have been studies that looked at PD-L1 positive vs. negative tumors and have demonstrated that those patients that have PD-L1 positive tumors have better clinical outcomes (as measured by overall response rate). However, while PD-L1 positive tumors show higher response rates to therapy versus PD-L1 negative tumors, biomarkers remain unreliable. PD-L1 negative tumors can still respond to treatment, and therefore we expect patients with PD-L1 negative tumors to be eligible for treatment. There are clinical trials directed against only PD-L1 positive tumors and those being run independent of PD-L1 status to help answer the biomarker question – but it remains open ended to date. Jami Rubin Winners and Losers If the initial data remains promising in later-stage clinical trials, there will clearly be winners and losers. It is not unrealistic to think that immuno-oncology agents could be used similarly to how US Pharma analyst email: Tel: [email protected] +1-212-357-7536 Goldman, Sachs & Co PD-1/PD-L1 phase 3 (phase 2) potential registrational studies Phase Identifier Tumor type Treatment line Comparator Patients Est. Primary Completion Date 3rd line 2nd line 2nd line 2nd line (Yervoy failures) 1st line 2nd line 1st line n/a Taxotere Taxotere 100 264 574 Feb-14 Aug-14 Nov-14 dacarbazine or carboplatin and paclitaxel 390 May-15 410 822 915 Sep-15 Feb-16 Oct-16 495 Jan-17 780 Mar-18 BMY 2 3 3 NCT01721759 NCT01642004 NCT01673867 Squamous NSCLC Squamous NSCLC Non-squamous NSCLC 3 NCT01721746 Metastatic melanoma 3 3 3 NCT01721772 NCT01668784 NCT01844505 Metastatic melanoma RCC Metastatic melanoma 3 NCT02041533 Recurrent/Stage IV NSCLC, PD-L1+ 1st line 3b/4 NCT02066636 Advanced/Metastatic NSCLC 2nd line dacarbazine Afinitor w and w/o Yervoy Alimta, Taxol, Paraplatin, Platinol, or Gemzar n/a NCT01866319 NCT01704287 NCT01905657 Metastatic melanoma Metastatic melanoma NSCLC, PD-1L+ 1st line 2nd line 2nd line Yervoy chemotherapy Taxotere 645 510 920 Jul-14 Mar-15 Sep-15 NCT01846416 NCT02008227 NSCLC, PD-L1+ advanced/metastic NSCLC 1st line 2nd line n/a Docetaxel 100 850 May-15 Jun-18 MRK 3 2 2/3 ROG 2 3 Source: clinicaltrials.gov. Goldman Sachs Global Investment Research 15 Fortnightly Thoughts Issue 70 Interview with...Sir Michael Rawlins Sir Michael Rawlins is the President of The Royal Society of Medicine in the UK and previously served a 14-year tenure as Chairman of the National Institute of Health & Clinical Excellence (NICE). He is also an Emeritus Professor at the University of Newcastle-upon-Tyne. Hugo Scott-Gall: What is NICE’s role in the UK health system? And what is its relationship with pharmaceutical companies? Sir Michael Rawlins: NICE is an independent public body that was set up in the UK in 1999 in an attempt to defuse the so-called postcode lottery of healthcare, where the availability of treatments depended upon the NHS Health Authority area in which the patient happened to live. NICE publishes appraisals and guidelines on drugs and treatments based primarily on evaluations of efficacy and cost, i.e. whether or not they represent increased value for money versus alternatives. Economic circumstances in the UK have meant that the government cannot always afford to pay the large sums of money required or demanded by the pharmaceutical industry. For drugs to be approved they have to be at a price that's affordable and that represents value for money to the tax-payer. This means healthcare systems constantly have to make difficult decisions; they cannot spend significant amounts of money on one drug for a small number of people as this disadvantages many others going without care. However, that being said, overall only 15% of products are rejected by NICE, with two-thirds accepted within their full license indications and the remaining restricted to use in certain subgroups of patients. In one sense, NICE is an extra hurdle in the process, but necessary in deciding the affordability of a new treatment relative to the benefits it brings for countries where healthcare is the responsibility of the state. NICE also plays an important role in pioneering technology assessments internationally. European countries such as Germany, France and Sweden have looked at the approaches that NICE has taken and are adapting them to their own countries circumstances. Essentially, all countries face the same problems of meeting increasing demand with finite, or sometimes diminishing resources. Hugo Scott-Gall: Who should be in the driving seat of innovation? Is it private companies for the revenue opportunity or governments to counter healthcare costs? Sir Michael Rawlins: There are massive areas of unmet need, particularly in the neurodegenerative area of diseases such as Alzheimer’s, Parkinson’s, and Huntington’s, where there is nothing that changes the course of the disorder. That requires a combination of private and public money to make discoveries, create new compounds and develop them into medicines. Publiclyfunded research, including trusts and universities, has played a very significant part over the years in the discovery process, but it needs the pharmaceutical industry to develop the products. However, in some cases, there is market failure as there may not be any incentives in place for pharma companies to develop new solutions. For instance, in antimicrobials and antivirals, the resistance to present-day antibiotics is causing real concern. The problem is that a pharmaceutical company would not go into Goldman Sachs Global Investment Research development because the minute the solution went onto the market, it would be heavily restricted by healthcare systems around the world to stop people from developing further resistance. Nevertheless, there are encouraging signs of collaboration. Recent examples include the European Union adding some €150 million into a joint anti-microbial research project with pharma companies in an effort to get pre-competitive programmes off the ground. Also, in the US it was announced that the National Institute of Health (NIH) is partnering with ten biopharmaceutical companies and contributing US$119 mn and US$111 mn respectively over the course of five years to focus on a handful of diseases for which there is currently no cure. There are massive areas of unmet need, particularly in the neurodegenerative area of diseases such as Alzheimer’s, Parkinson’s, and Huntington’s, where there is nothing that changes the course of the disorder. That requires a combination of private and public money to make discoveries, create new compounds and develop them into medicines. Hugo Scott-Gall: Which areas across the healthcare spectrum do you feel most excited and optimistic about in terms of breakthroughs? And how do you think about technology and Big Data in particular? Sir Michael Rawlins: There is the potential for significant progress as a result of us knowing more about the biology of diseases. Being able to identify more targets that are tractable should give a rise in the quantity of new medicines and lead to improvements in their safety. This has most widely been true in cancer, but currently most of the anti-cancer products have served to provide extensions of life by a few months but have not actually fulfilled their promises of bringing cures, which is what we want. Will Big Data make a difference? The answer is yes it certainly is improving efficiency in the regulatory framework. Presently, the European Medicines Agency (EMA) has been discussing introducing adaptive licensing which involves receiving earlier authorization for certain new drugs and gathering real-time data on an ongoing basis to evaluate results. Companies are currently completing Phase 2 studies and are waiting to go onto Phase 3 - a process which can take over 10 years to complete. However, in the future if a product finishes Phase 2 and is particularly promising it could receive conditional authorization. These types of initiatives are worth pursuing because anything that reduces the length of time before a drug gets on the market has two advantages. First, it gives patients an opportunity to benefit from it; and secondly, if it shortens the period of drug development it'll reduce the cost. Hugo Scott-Gall: In publicly funded healthcare systems, what are the factors apart other than cost that feed into the equation of approving some treatments? 16 Fortnightly Thoughts Sir Michael Rawlins: There is a lot of talk, especially in the UK, about what's been known as value-based pricing - where setting prices is primarily based on the estimated customer utility rather than on historical prices or cost of product. This is a tricky subject as this means different things to different people. It’s a question of the extent to which you extend the value of a pharmaceutical product beyond the healthcare system. Should you, for example, include what economists have called a productivity benefit, i.e. when people can go back to work rather than be laid off by the disability or illness. Inevitably, these tend to be political questions with less than straightforward answers. For example, the disadvantages of factoring in a productivity component for a country like the UK is that it isn’t all that compelling when there is a 7% unemployment rate. A second problem is that in the UK, the productivity idea would almost certainly be in conflict with the Equality Act because it inherently creates an advantage for people who are in employment and disadvantages for those not employed, particularly the elderly. Any such decision would almost certainly be stumped at the judicial review. In other countries too, it would be very difficult for any politician to reduce the amount of care on the elderly as they’re the ones who come out and vote. They also account for a big proportion of consumption in an economy. If we were to take a wider societal perspective and look at productivity, then yes, the elderly would be disadvantaged. So, for most countries, there are two components to look at here – how constrained is the healthcare system and the extent to which they want to take the benefits into account. Both are political decisions which different implications in different countries. The other issue is that these decisions are not based on analysis that gives us a straight yes or no answer, and they depend heavily on the social values very specific to countries. For instance, should we assess drugs for very rare diseases in the same manner given that they are always going to be much more expensive than the drugs for common ones? We can't just translate the social values we've adopted at NICE and put them into Italy or Spain, let alone Thailand, Burma or Brazil. What I think will happen is that the scientific methodologies may converge in different countries. But it will still be individual countries that make their decisions depending on their economic circumstances, depending on their social values, depending on their political climate. I can understand how troublesome it must be for companies to have to produce 29 different submissions for each member state in the European Union. Hugo Scott-Gall: What is NICE’s and the UK’s influence on global healthcare systems? Sir Michael Rawlins: Developing countries are very interested in health technology assessment because they have to assess priorities in their healthcare systems too. How much they have to pay relative to what they get for the money is becoming a very important component. Our appraisal programme has been easier for us to export as the UK has a long tradition of evaluation, Goldman Sachs Global Investment Research Issue 70 comparative effectiveness research and health economics. In particular, we appreciate the influence of the York School of Health Economics, which has worked on the effects of decisions the NHS has taken on specific services and what they have meant for the length and quality of life. They track real overall expenditure and productivity which encourages accountability in the system, but also predictability for investment decisions. At NICE, all the members of our guideline groups are completely independent of any sort of interest. Of course manufacturers are entitled to have their say, but they don't necessarily have their way. Hugo Scott-Gall: And how about the US, are we likely to see global protocols? Sir Michael Rawlins: It is more difficult in the US as many North American clinical guidelines are over-influenced by sponsorship by big pharmaceutical companies. This is not just my assessment but other Americans are talking about it; the editor of the journal, JAMA, has voiced strong concerns as well. At NICE, all the members of our guideline groups are completely independent of any sort of interest. Of course manufacturers are entitled to have their say, but they don't necessarily have their way. Hugo Scott-Gall: Apart from drugs, in which other parts of the healthcare value chain do you see potential for better cost efficiency? Sir Michael Rawlins: We shouldn’t forget that approximately 70% of healthcare costs are from the people the industry employs doctors, nurses, pharmacists and so on. We are not going to make too many inroads into lowering costs in those areas without having an impact on the quality of care. In the UK and the NHS, the gains are going to be made in two areas. The first is the need to re-engineer services, so that there are fewer clinics but more concentrated services for an assortment of trauma, accident and emergency ailments. The second is that care has to be developed and more integrated across primary and secondary care. Both of these areas are going to be tricky to redesign. Re-engineering services is difficult because, for example, in Bournemouth and Poole, merging hospitals on perfectly sensible grounds attracted attention from the competition commission. Integrating primary and secondary healthcare is also going to prove to be difficult as there are currently separate commissioning arrangements for both. Primary care is commissioned by the regional team and the clinical commissioning group commissions secondary care. 17 Fortnightly Thoughts Issue 70 Making the case for stem cells Andrea Chong, from our Australian Healthcare team, explores the potential in stem cells Stem cells are the body’s cellular building blocks from which nearly all other cells are formed. They are important in the repair and replacement of damaged cells and hold remarkable promise for many of the world’s most serious diseases. Here, we focus on the latest milestones achieved by stem cell research and explore a number of areas where it could be potentially disruptive for current treatment regimes. What are stem cells and what makes them special? Scientists have made great progress in isolating many different types of stem cells and uncovering how they work, although a lot remains to be understood. As the body’s basic cellular material, stem cells are understood to have two distinct properties. First, they are capable of self-replication. Second, they can develop into a range of specialised cell types, including bone, blood vessels, neurons, muscle and cartilage. Recent research has also shown that they could play a role in improving the function of the specialised cells around them, and may have anti-inflammatory and immunosuppressive properties. The possibilities of clinical applications are seemingly endless. Current clinical uses of stem cells are still very limited Despite the attention surrounding their potential, the range of diseases for which stem cells are currently approved is extremely limited. In the field of hematology and oncology, doctors have been using hematopoietic (blood) stem cell transplantation for over 50 years as standard treatment for certain cancers and immune system disorders such as leukemia and lymphoma. Apart from this, a number of companies (two in the US, one in Korea, one in Europe) have been selling stem cells to patients for wound repair, cartilage repair and bone graft material, but on a small-scale, bespoke basis only and hence subject to limited regulatory review. In the US, blood stem cell transplantation is the only FDA approved use for stem cells. Another recent and related development has been the rise in popularity of private cord blood banking, which is the collection and preservation of stem cell-rich umbilical cord blood for possible later use. No verdict yet on efficacy; but could be commercially viable Embryonic stem cells vs. adult stem cells. Scientists have known about the existence of stem cells for at least a century but it has only been since the late 1990s, when human embryonic stem cells were first cultured in the laboratory, that stem cells have been viewed as a potential form of treatment. However, much of the discussion on stem cells then was focused on the intense ethical debate around the destruction of human embryos for stem cell harvesting. Today, embryonic stem cell research is still conducted in many parts of the world but is highly regulated. Given the controversies, future uses in the clinic appear very unlikely. To side step the ethical issues associated with embryonic stem cells, scientists are now focused on the potential of adult stem cells. Although much less potent, adult stem cells, obtained in many cases from the bone marrow of healthy donors, provide an accessible alternative to embryonic stem cells. Emerging signs of commercial viability. A key achievement of stem cell research in the last decade has been to show that certain types of adult stem cells in certain types of settings are, at least, safe for use in the human body – although we do note that patient Goldman Sachs Global Investment Research sample sizes have been small to-date (typically less than 100). Nonetheless, this is an extremely important milestone given concerns around potential tumour/cancer formation, infection and immune system rejection. Related to this is the ability to grow stem cells in large numbers rapidly and cost-effectively to unlock their “off-the-shelf” commercial potential. Scientists initially explored the use of the patient’s own stem cells, termed autologous stem cells, to reduce the chance of immune system rejection but their commercial viability is limited because their manufacture is not easily scalable (given the need to harvest and grow the cells before re-transplanting into the patient). Instead, scientists have now successfully isolated and identified a few types of allogeneic stem cells (meaning stem cells originating from a different person and hence genetically dissimilar), which do not appear to illicit an immune system response in the recipient. Of these stem cells, the most promising type appears to be mesenchymal (meaning connective tissue) stem cells, or MSCs. MSCs can be extracted from a small number of healthy donors, usually from the bone marrow, and then significantly expanded and reproduced for potential use in thousands of patients. Because MSCs do not require tissue-type matching to the patient, which can be a time-consuming process, they can also be extremely valuable for acute/emergency uses. Publicly traded stem cell companies Led by Australian stem cell company, Mesoblast (market capitalisation A$1.9 bn), there are approximately 20 public and private companies active in stem cell development. Roughly half of these companies use autologous stem cells and half use allogeneic stem cells. Many use MSCs. Others use stem cells from fat tissue (via liposuction), human placenta, or a human fetus. Of these companies, Mesoblast has the most comprehensive clinical trial programme with late-stage trials about to commence in heart failure (funded by Teva Pharmaceuticals) and intervertebral disc repair for back pain. The company also expects to make a regulatory submission to the FDA on pediatric graft versus host disease in the next 12 months, which if successful, could be the first FDAapproved stem cell product available for sale in the US. Market Capitalisation (US$ mn) STEM CELL THERAPEUTICS CORP (CA) RENEURON GROUP PLC (GB) STEM CELL THERAPEUTICS CORP (CA) ADVANCED CELL TECHNOLOGY INC (US) NEOSTEM INC (US) TIGENIX NV (BE) CYTORI THERAPEUTICS INC (US) BIOTIME INC (US) PLURISTEM THERAPEUTICS INC (IS) NEURALSTEM INC (US) ATHERSYS INC (US) STEMLINE THERAPEUTICS INC (US) MEDIPOST CO LTD (SK) OSIRIS INC (US) MESOBLAST LTD (AU) $0 $200 $400 $600 $800 $1,000 $1,200 $1,400 $1,600 $1,800 Source: Goldman Sachs Global Investment Research, Bloomberg. Future disruptive potential? We highlight three areas where stem cells could be potentially disruptive for currently available treatments – noting, of course, that these three examples represent only the tip of the iceberg. There is a vast body of research exploring stem cells in a range of other diseases including cerebral palsy, diabetic kidney disease, multiple sclerosis and blindness. 18 Fortnightly Thoughts Where can we use stem cells? Issue 70 mn) makes one of the few commercially-available stem cell products in the world, although its availability is limited only to Korea. Its product uses MSCs obtained from umbilical cord blood and is used to repair cartilage damage in the knee caused by osteoarthritis. Another company, Belgium-based Tigenix (market capitalization US$200 mn) has a similar product that is available in the EU but uses autologous, not allogeneic, stem cells. Its product was the first cell-based product to be successfully approved in the EU under its Advanced Medicinal Therapy Programme in 2009. Australian-based Mesoblast is looking to treat diseases of the spine. The company recently reported results from a 100 patient trial in intervertebral disc degeneration showing that an injection of its stem cells into a damaged intervertebral disc, improved both back pain and disc stability. If later-stage trials are successful, Mesoblast could have a commercially available product for back pain by 2016. Stroke Source: Goldman Sachs Global Investment Research. Cardiovascular diseases One of the largest opportunities for stem cells is in cardiovascular diseases, given their large global prevalence in the population. Mesoblast, together with partner Teva Pharmaceuticals, is about to commence a large (1,700 patients) Phase III trial investigating the use of stem cells in heart failure, which is characterised by weakened heart muscle most likely due to a prior heart attack or hypertension. Current available treatment for heart failure includes heart stents, medications, coronary bypass surgery or, in end-stage cases, heart transplants. In Mesoblast’s trial, stem cells are injected via catheter into the damaged heart muscle. The stem cells are designed to release factors to induce blood vessel formation, heart muscle regeneration and reduce scarring; hence improving heart function and ultimately, mortality. Previous trials in 45 patients showed positive signs on both heart muscle strength and mortality measures. While a number of animal studies have shown that stem cells can improve cognitive function after a stroke, the research in human patients is still in early stages. Stroke is the single largest cause of adult disability in the world and there are very few treatment options available to patients. One company at the forefront of stem cell research in stroke is UK-based Reneuron (market capitalisation £60 mn) which uses neural stem cells from a fetus that are genetically engineered and then expanded in culture. All nine patients in its study demonstrated reductions in neurological impairment, with most sustaining the improvements in the longer term. The company plans to commence Phase II trials this year, subject to regulatory approval. The next three to four years are exciting ones for the stem cell industry. In that time, we may have persuasive evidence that certain types of stem cells could be effective in some medical applications, and we would be another few steps closer to uncovering its full clinical potential. Andrea Chong, CFA Orthopedic diseases Australia Healthcare analyst There is a significant body of research on the use of stem cells in orthopedic diseases. Currently, there are limited curative options for these diseases with most treatments targeted at symptomatic relief. Korean-based company Medipost (market capitalization US$435 email: Tel: Goldman Sachs Global Investment Research [email protected] +61-3-9679-1126 Goldman Sachs Australia Pty Ltd 19 Fortnightly Thoughts Issue 70 China: Insurance key for healthcare reform Our China Healthcare analyst, Wei Du, PhD, argues that the success of hospital reform hinges on insurance reform In just 20 years, China has risen from outside the top 10 healthcare markets in the world to being the third largest. Rising incomes, an ageing population and increasing demands for quality care look set to drive further growth in healthcare spending. However, a deteriorating dependency ratio, increasing patient awareness and the prospect of the government assuming a greater share of spending looks set to increase the focus on the value and quality of healthcare provision. To meet growing expectations, we believe that the government will need to provide a market structure that incentivises the provision of effective, safe and low-cost medical services. We envisage drug prices, notably branded generics, continuing to drop, and see insurance reform as increasingly imminent as all incentives hinge on an efficient payer system. Insurance reform is key to the success of hospital reform 1. Hospital reform taking centre stage In 2013, the Third Plenum laid out a more market-based healthcare reform blueprint, with three major changes: (1) further drug price control, driven by essential drug lists (EDLs) expansion: (2) “deadministration” of public hospitals, and encouragement of private investment in the healthcare service sector; and (3) centralised control of urban/rural medical insurance and its gradual extension to private hospital coverage. While the overarching relationship of patient, provider (e.g. hospitals) and payer (e.g. the government, insurance companies) is a delicate balance, we believe insurance reform is key to the success of hospital reform. China’s healthcare reform Insurance reform is a key limiting step Insurance reform: Breaking the de-facto Payer-Provider alliance is key for the welfare of patients Insurance reform is a key limiting step • Subject to hospital prescriptions, little bargaining power Patient Payer (Insurance provider) • Little third-party basis to argue for payment • De-facto alliance with Provider • Bear most cost risk • Excluded from defacto Payer-Provider alliance Provider (Hospitals) • Sole determinant of medical cost, profitability linked to higher medical cost on patient • No incentives to control high costs Source: Gao Hua Securities Research, China National Health and Family Planning Commission. 3. Changing payer and provider relationship to ensure a fair, efficient healthcare system to ultimately serve patient’s need We believe that correcting the payer/patient relationship and better aligning insurance payout schemes with the provision of quality healthcare services is key to China healthcare reform, and enhancing China’s social welfare system. We consider the following as of paramount importance over the next 3-5 years: • Expansion of insurance coverage to major illnesses and increasing use of private hospitals. • Centralised third-party insurance management programme to achieve cost reduction. Integration of the Urban Basic Medical Insurance Program (UBMI) and New Rural Cooperative Medical Scheme (NRCMS) is the first step, and should lead to improved affordability of healthcare services as well as hospital efficiency. • Development of a DRG system to standardize medical practice and minimize redundancy to improve overall service efficiency. Source: Gao Hua Securities Research, China National Health and Family Planning Commission. 2. Loopholes in China’s the three “Ps” relationship The three “Ps” in China are poorly aligned to some extent: (1) with few private insurance companies in play, payers in China are in the main a government body whose primary focus is cost. This does not serve the patients’ best interest in terms of service quality; (2) as a government entity, China’s payer also aims (in part) to support service providers, i.e. hospitals, as both are under the supervision of the Ministry of Health. This can lead to less scrutiny on physician’s practice, inflated costs owing to a high level of service redundancy, and limited patient choice or bargaining power. • Growing commercial private insurance to serve broad needs helped by broader scope of investment vehicles. • Insurance payments should shift from a fee-for-service model to measures based on performance and economic outcomes. Emerging hospital chains/management group Ongoing hospital reform will likely create a hospital chain and large hospital management group in the near to medium term in our view. With increasing policy support for healthcare service providers, we see: • Growing interest in investing in China’s healthcare service sector, which we expect to offer stable growth and strong cash flow in the long term, as Chinese patients often pay upfront before seeking medical treatment. • Encouragment of private investment in public hospitals, helped by “de-administration”in China’s public hospitals. Goldman Sachs Global Investment Research 20 Fortnightly Thoughts Issue 70 • Changing hospital revenue mix towards services, rather than relying heavily on drug sales. Government is taking up a larger role in healthcare expenditure, thanks to broader insurance coverage • Improving service efficiency and quality, via sharing resources among a group of hospitals, and developing proper incentive schemes to motivate medical practitioners. Individual, society and government annual healthcare expenditure as % of total annual healthcare expenditure in China Government • Hospital groups/chains, at some point, might serve as major service entities to cooperate with insurance providers to better serve the social function. Society Individual 100% 90% 80% 25.1% 18.0% 17.9% 18.1% 29.9% 35.6% 24.7% 27.5% 28.6% 30.4% 35.1% 35.9% 34.7% 40.4% 37.5% 35.5% 34.9% 2008 2009 2010 2011 32.6% 33.6% 60% Number of public and private hospitals (2003 -9M2013) 22.3% 25.6% 70% Private hospitals are on the rise, taking share from public ones 15.5% 36.2% 39.2% 34.9% 50% # of private hospitals # of public hospitals Private hospital as % of total hospitals 40% 14,000 13,427 50% 44.6% 30% 45% 20% 12,000 10,795 10,000 40% 35% 10% 25% 6,000 59.0% 46.4% 52.2% 49.3% 44.1% 35.7% 21.2% 0% 1980 30% 8,000 42.6% 1990 1995 2000 2005 2006 2007 Source: National Health and Family Planning Commission (NHFPC). 20% 10% 2,000 5% 0% Sep-13 Jul-13 Aug-13 Jun-13 Apr-13 May-13 Mar-13 Feb-13 Oct-12 Nov-12 Sep-12 Jul-12 Aug-12 Jun-12 Apr-12 May-12 Mar-12 Feb-12 Oct-11 Nov-11 Sep-11 Jul-11 Aug-11 Jun-11 Apr-11 May-11 Mar-11 0 Source: National Health and Family Planning Commission (NHFPC). Increasing government funding and insurance expansion are leading to rising demand for service efficiency and quality, and a regulatory constraint on public hospital expansion offers significant opportunities for private hospitals in the next 3-5 years. The number of private hospitals has been growing at an 18% CAGR (2003-12), reaching 10,795 by the end of September 2013 and accounting for 45% of the 24,222 hospitals in China. However, the number of beds in private hospitals (2012) is just 10.2% of total hospital beds, at 0.58 mn vs. 5.14 mn beds in public hospitals. Independent clinical labs (ICLs) and pharmacies, the next contenders With the introduction of more private hospitals and clinics, comes demand for services such as independent clinical labs (ICLs) and pharmacy management. Compared with the c.40% penetration rate of ICLs in the US, China’s ICLs have less than 2% market share. With ICLs’ expertise, focus and centralisation, we see more hospitals, private or public, having the incentive to outsource their clinical lab services to ICLs, to save cost and improve efficiency. We favour the emerging independent clinical labs (ICLs) as we see them as able to take a significant share of the testing/diagnostic businesses from the clinical laboratory departments of hospitals by offering a wider service portfolio and more cost-effective and timely diagnostic services to hospitals of all sizes. With a heightened scrutiny on over-subscription of drugs, and widespread “zero mark-up” policies for hospitals, to cut their dependence on drug revenues, China’s healthcare reform is increasingly tilting towards disease prevention. This drives demand for diagnostic services, benefiting independent clinical labs (ICLs) and, to a larger extent, medical devices companies that make in-vitro diagnostic (IVD) products in our view. Goldman Sachs Global Investment Research Evolving market dynamics; stay selective Despite a cost containment policy, the long-term growth potential of the sector will remain mid-teens for the next 5-10 years in our view, driven by favourable demographic trends, economic development, new product launches and government insurance expansion. The healthcare service sector should continue its strong momentum, tapping more private capital with the implementation of more market-based reform. However, we expect a major shift from pure EPS growth to core competence to the ability to deliver sustainable growth, which might be reflected by fruition of R&D pipeline, abundant capital, and stronger wave for M&A as a driver for growth in diverse businesses. A roaring decade continues… Shenyin Wanguo (SWS) A-share healthcare index 1999-2004 CAGR 2% 2004-2009 CAGR 16% SWS A-share 300 Index 2009-2014 CAGR 18% 500% 400% 300% 200% 100% 0% -100% Dec-99 May-00 Oct-00 Mar-01 Aug-01 Jan-02 Jun-02 Nov-02 Apr-03 Sep-03 Feb-04 Jul-04 Dec-04 May-05 Oct-05 Mar-06 Aug-06 Jan-07 Jun-07 Nov-07 Apr-08 Sep-08 Feb-09 Jul-09 Dec-09 May-10 Oct-10 Mar-11 Aug-11 Jan-12 Jun-12 Nov-12 Apr-13 Sep-13 15% 4,000 Source: Goldman Sachs Global Investment Research. Wei Du, Ph.D China Healthcare analyst Email: Tel: [email protected] +86-21-2401-08928 Beijing Gao Hua Securities Company Limited 21 Fortnightly Thoughts Issue 70 The 3D printing revolution in medical devices Our European MedTech analyst, Veronika Dubajova, discusses the 3D printing revolution in medical devices Personalized medical devices represent a growing trend in the healthcare space. While their use was historically restricted to oneoff cases in patients with difficult anatomy, recent advances in manufacturing technologies such as 3D printing and CAD/CAM have enabled sizeable parts of the medical device industry to move towards automated manufacturing of customized devices, often at a lower cost. Personalised medical devices are largely superior to standard-sized ones: since they are specifically tailored to the patient's anatomy, they fit better (there’s no such thing as a normalsized ear canal) and therefore improve the outcome for the patient. In some cases, the use of personalised devices or instrumentation can even drive down the cost of the procedure, as is the case for personalised instrumentation in orthopaedics. Importantly, recent technology advances suggest that over time 3D printing could be used to not only manufacture one-off tailored medical devices, but also to lower manufacturing costs for standard implants, and in the medium term, to print human tissues, and potentially human organs, opening up significant possibilities for drug development, testing, and, in the long term, organ transplantation. Here, we explore the current use of 3D printing in medical device manufacturing, and the disruptive potential this technology has in the medium and long term in our view. Increasing productivity: Using 3D printing to make personalised hearing aids The hearing aid industry was an early adopter of 3D printing, with most of the industry now using it to manufacture patient-specific inthe-ear hearing aids; we estimate that over 80% of in-the-ear hearing aids are 3D-printed today, from 20% seven years ago. The move towards 3D printing has many advantages: it has driven higher productivity for hearing aid manufacturers (custom in-the-ear hearing aids were previously made by hand, using injection moulding techniques), and has significantly improved the fit of the hearing aid for the patient, resulting in a higher comfort level. In recent years, 3D printing has also allowed hearing aid makers to move to more sophisticated materials, which are thinner but harder, driving further miniaturisation and creating hearing aids that sit so deep in the ear canal, they are almost invisible. Automating a once-manual process: Using CAD/CAM for dental restorations CAD/CAM (computer-aided design and manufacturing) has been used for manufacturing dental restorations for over 20 years, but has only gained popularity in the past 5-10 years, as the technology became more affordable, the software easier to navigate, and its use expanded from dental laboratories to dentist’s offices. The principle of CAD/CAM is akin to 3D printing – the dentist takes a physical or digital impression of the patient’s teeth, which is manipulated to create a digital version of a dental restoration (such as an onlay or crown), and milled either locally or centrally in a large milling facility, depending on complexity. The key advantage of a CAD/CAM-made restoration is speed; a CAM machine can mill an onlay in 2-5 minutes, versus the lab’s approximately two hours to complete the same process by hand, though, at least today, CAD/CAM-made restorations are still slightly more expensive than hand-made ones, given the need for better materials. Goldman Sachs Global Investment Research 3D printing has driven higher productivity for the hearing aid manufacturers Revenue and employee growth, indexed to 2005 220 200 180 160 140 120 100 2005 2006 2007 2008 2009 2010 2011 William Demant - revenues William Demant - manufacturing salaries Sonova - revenues Sonova - manufacturing employees 2012 Note: Revenue growth includes acquisitions. Source: Company data. The growing use of CAD/CAM has had profound effects on the dental laboratory industry, where the number of dental labs has declined by 30% over the past five years, as the industry has consolidated given higher productivity. Penetration of chari-side milling (CAD/CAM) by territory 18% 16% 14% 12% 10% 8% 6% 4% 2% 0% Switzerland Germany US Australia Rest of Europe Japan Source: Goldman Sachs Global Investment Research. Driving savings: Using personalised instrumentation in total knee replacements Patient-matched instrumentation is a relatively new technology in orthopaedics; it uses either an MRI or CT scan to manufacture a disposable cutting block which is then used to guide the surgeon during the procedure. Aside from better patient outcomes, personalised instrumentation has other significant benefits: it reduces surgery time, potentially driving higher operating room throughput, and shortens the duration of hospital stay, lowering costs per patient. Most importantly, personalised instrumentation lowers the number of instrumentation trays required during the surgery, which results in efficiencies for the hospital (such as lower sterilization costs per procedure) and the device manufacturer (lower capital investment). We estimate that around a quarter of knee replacements in the US utilise patient-matched instrumentation today, up from 0% five years ago, though we expect this to rise significantly over the coming years. 22 Fortnightly Thoughts Patient-specific products to lowering manufacturing costs: 3D printing to manufacture standard implant components To date, 3D printing has played an important role in manufacturing one-off, patient-specific devices and implants, enabling a greater degree of personalisation, and therefore, a better fit for patients in certain settings. However, over the last 12-18 months, some medical device manufacturers have begun exploring how 3D printing could be used day-to-day to manufacture standard implant components at a lower cost, and potentially with better patient outcomes. Stryker and Smith & Nephew now both use 3D-printing to manufacture certain components of knee replacements (tibial plates), as the technology allows them to produce a rougher surface that is more suitable to bone in-growth (i.e. osteoconductive), which in turn increases the implants’ stability. While the use of 3D printing for manufacturing of standard-sized implants is still in its infancy – the companies currently use the technology only for one specific implant component – both Stryker and Smith & Nephew believe that in certain cases, 3D printing could not only lead to producing superior products, but also to lowering manufacturing costs, given less waste (today, most implants are made using subtractive manufacturing, wherein an object is carved from a material such as metal, plastic and ceramic, which leads to wasted material that will not be used for the implant). While we do not expect 3D printing to become the industry’s manufacturing technology of choice, we believe that it offers advantages for certain products, and will therefore be adopted more widely in the medium term, potentially driving manufacturing costs lower. From metal and plastic to living tissues: 3D bioprinting For years, tissue engineers have tried to produce lab-grown human tissues robust enough to serve as replacements for damaged human tissue, with limited success, though 3D printing appears to be offering a solution. 3D printing excels at creating intricately detailed 3D structures, typically from inert materials like plastic or metal. 3D printing’s ability to create intricately detailed structures is particularly useful for tissues inside the human body, which contain multiple cell types that are often arranged into a specific pattern or structure, driven by the functions required of that tissue. For example, a human blood vessel has three distinct cellular layers; a thin outer fibrous coating, composed of fibroblast cells and their extracellular matrix; a media, composed of smooth muscle cells that can expand and contract in response to physical or chemical stimuli, and a thin inner layer of endothelial cells that line the lumen of the vessel and act as a barrier between the blood and underlying tissue. 3D bioprinting enables this complex construction of tissues layer by layer, ensuring that each layer contains the relevant cell types and has dimensions that approximate those of native tissue. While commercial distribution of 3-D printed organs for transplantation remains far off, companies and research institutions are taking steps in that direction with distribution of printed organs for research use due to begin over the next 1-2 years. In fact, Organovo – one of the commercial human tissue manufacturing Goldman Sachs Global Investment Research Issue 70 companies – expects to start selling liver tissue to drug developers over the next 1-2 years. There are many advantages to testing compounds on organs made of human tissue: rodents have slightly different enzymes, which means that they do not always react the same way to drugs. For example, if the enzymes in the rodent liver do not modify the drug, the compound may remain inactive even though it is efficacious in humans. What’s going on ‘ear’ then? Source: Company presentation. Long term, 3D bioprinting could not only enable us to print human tissues for testing and potentially human organs for transplantation (e.g. liver and kidneys), but could also allow us to “construct” functional organs that merge electronics and human tissues. For instance, last year, researchers at Princeton University 3D-printed a “bionic ear”, combining bio-printed organic materials and electronics. The ear consisted of a coiled antenna inside a cartilage structure, and while not yet suitable to be used on a patient, it lays the groundwork for one that could be used to restore human hearing (the electrical signals produced by the ear would be connected to a patient's nerve endings, like a cochlear implant). 3D printing offers a range of exciting, and potentially transformative solutions to multiple problems in the human body. Personalized devices are a growing trend, and their use will likely increase as 3D printing becomes more widely adopted. 3D printing should also be more widely used in the manufacturing of certain standard-sized implant components, potentially lowering manufacturing costs. Long term, 3D bioprinting could meaningfully transform drug development and increase our ability to replace human tissues and organs, lowering the cost of care for critically ill patients today. Veronika Dubajova European MedTech analyst email: Tel: [email protected] +44-20-7774-1901 Goldman Sachs International 23 Fortnightly Thoughts Issue 70 Six of the best – our favourite charts In our six of the best section, we pull together a pot pourri of charts that we hope you will find interesting. They will be different in each edition but hopefully always of note. Happier Danes, gloomier Chinese The ARM army Deviation of consumer confidence index from long-term average Percentage of world’s population that… Avg 2012 Avg 2013 70% Latest 3 60.0% 60% 59.9% 2 52.6% 50.0% 50% 1 0 40% 35.6% -1 30% -2 -3 20% -4 10% China France US Japan Italy Spain Netherlands Australia Finland Switz. Germany S.Korea UK Sweden Denmark -5 0% Uses an "ARM" based device daily Is employed (for age 15+) Lives in an urban Has an account at a area formal institution (for age 15+) Source: OECD. Source: World Bank, Bloomberg Businessweek. Kicking off Tweets from the throne Top 10 kickstarter campaigns by the amount of money raised since inception Number of heads of state who tweet globally Initial goal 140 Total raised Pebble (customizable E-Paper watch for iPhone and android) Has access to internet 133 (80%) 123 (75%) 120 OUYA (Android based game console) Veronica mars movie project (Independent film) 100 Torment (game) Project eternity (game) 80 69 (42%) Wish I was here (Independent film) 60 Form 1 (High res. 3D printer) Oculs Rift (Virtual; reality headset for video games) 40 33 (20%) 3Doodler (Pen that can draw in the air) Emotiv Insight (Wireless headset that monitors and records brain activity data) 20 - 2,000 4,000 6,000 8,000 10,000 12,000 0 2010 2011 2012 2013 Source: Bloomberg. Source: DigitalDaya. Instant feedback Not as tight as you think Following M&A announcement, % of companies whose share price increased and average 1-day price performance of all firms. Estimated 10-year BBB Industrial spread to Treasury 70% 0.8% 0.7% 60% 0.6% 0.5% 50% 0.4% 40% 0.3% 8 % of acquirers that saw share price increase on day 1 (LHS) 0.2% 30% 0.0% -0.1% 10% 75th %ile 25th %ile 7 6 5 4 0.1% 20% Estimated 10-yr BBB Industrials spread Median All-time tight Average 1 day share price performance (RHS) 3 2 1 -0.2% Source: Bloomberg. Goldman Sachs Global Investment Research 2012 2008 2004 2000 1996 1992 1988 1984 1980 1976 1972 1968 1964 1960 1956 1952 0 1948 2014 1944 2013 1940 2012 1936 2011 1932 2010 1928 2009 1924 2008 1920 -0.3% 0% Source: Moody’s, S&P, Haver Analytics, Goldman Sachs Global Investment Research. 24 Fortnightly Thoughts Issue 70 Disclosure Appendix Reg AC We, Hugo Scott-Gall, Sumana Manohar, Keyur Parekh, Steve Chesney, Eleanor Fung, Mick Readey, Isaac Ro, Jami Rubin, Andrea Chong, Wei Du and Veronika Dubajova, hereby certify that all of the views expressed in this report accurately reflect our personal views about the subject company or companies and its or their securities. We also certify that no part of our compensation was, is, or will be, directly or indirectly, related to the specific recommendations or views expressed in this report. Investment Profile The Goldman Sachs Investment Profile provides investment context for a security by comparing key attributes of that security to its peer group and market. The four key attributes depicted are: growth, returns, multiple and volatility. Growth, returns and multiple are indexed based on composites of several methodologies to determine the stocks percentile ranking within the region's coverage universe. The precise calculation of each metric may vary depending on the fiscal year, industry and region but the standard approach is as follows: Growth is a composite of next year's estimate over current year's estimate, e.g. EPS, EBITDA, Revenue. Return is a year one prospective aggregate of various return on capital measures, e.g. CROCI, ROACE, and ROE. Multiple is a composite of one-year forward valuation ratios, e.g. P/E, dividend yield, EV/FCF, EV/EBITDA, EV/DACF, Price/Book. Volatility is measured as trailing twelve-month volatility adjusted for dividends. Quantum Quantum is Goldman Sachs' proprietary database providing access to detailed financial statement histories, forecasts and ratios. It can be used for in-depth analysis of a single company, or to make comparisons between companies in different sectors and markets. GS SUSTAIN GS SUSTAIN is a global investment strategy aimed at long-term, long-only performance with a low turnover of ideas. The GS SUSTAIN focus list includes leaders our analysis shows to be well positioned to deliver long term outperformance through sustained competitive advantage and superior returns on capital relative to their global industry peers. Leaders are identified based on quantifiable analysis of three aspects of corporate performance: cash return on cash invested, industry positioning and management quality (the effectiveness of companies' management of the environmental, social and governance issues facing their industry). Disclosure Appendix Coverage group(s) of stocks by primary analyst(s) There are no coverage groups associated with the analyst(s). Company-specific regulatory disclosures The following disclosures relate to relationships between The Goldman Sachs Group, Inc. (with its affiliates, "Goldman Sachs") and companies covered by the Global Investment Research Division of Goldman Sachs and referred to in this research. Compendium report: please see disclosures at http://www.gs.com/research/hedge.html. Disclosures applicable to the companies included in this compendium can be found in the latest relevant published research. Distribution of ratings/investment banking relationships Goldman Sachs Investment Research global coverage universe Rating distribution Global Investment Banking Relationships Buy Hold Sell Buy Hold Sell 32% 54% 14% 53% 45% 36% As of January 1, 2014, Goldman Sachs Global Investment Research had investment ratings on 3,637 equity securities. Goldman Sachs assigns stocks as Buys and Sells on various regional Investment Lists; stocks not so assigned are deemed Neutral. Such assignments equate to Buy, Hold and Sell for the purposes of the above disclosure required by NASD/NYSE rules. See 'Ratings, Coverage groups and views and related definitions' below. Goldman Sachs Global Investment Research 25 Fortnightly Thoughts Issue 70 Price target and rating history chart(s) Compendium report: please see disclosures at http://www.gs.com/research/hedge.html. Disclosures applicable to the companies included in this compendium can be found in the latest relevant published research. Regulatory disclosures Disclosures required by United States laws and regulations See company-specific regulatory disclosures above for any of the following disclosures required as to companies referred to in this report: manager or co-manager in a pending transaction; 1% or other ownership; compensation for certain services; types of client relationships; managed/co-managed public offerings in prior periods; directorships; for equity securities, market making and/or specialist role. Goldman Sachs usually makes a market in fixed income securities of issuers discussed in this report and usually deals as a principal in these securities. The following are additional required disclosures: Ownership and material conflicts of interest: Goldman Sachs policy prohibits its analysts, professionals reporting to analysts and members of their households from owning securities of any company in the analyst's area of coverage. Analyst compensation: Analysts are paid in part based on the profitability of Goldman Sachs, which includes investment banking revenues. Analyst as officer or director: Goldman Sachs policy prohibits its analysts, persons reporting to analysts or members of their households from serving as an officer, director, advisory board member or employee of any company in the analyst's area of coverage. Non-U.S. Analysts: Non-U.S. analysts may not be associated persons of Goldman, Sachs & Co. and therefore may not be subject to NASD Rule 2711/NYSE Rules 472 restrictions on communications with subject company, public appearances and trading securities held by the analysts. Distribution of ratings: See the distribution of ratings disclosure above. Price chart: See the price chart, with changes of ratings and price targets in prior periods, above, or, if electronic format or if with respect to multiple companies which are the subject of this report, on the Goldman Sachs website at http://www.gs.com/research/hedge.html. Additional disclosures required under the laws and regulations of jurisdictions other than the United States The following disclosures are those required by the jurisdiction indicated, except to the extent already made above pursuant to United States laws and regulations. Australia: Goldman Sachs Australia Pty Ltd and its affiliates are not authorised deposit-taking institutions (as that term is defined in the Banking Act 1959 (Cth)) in Australia and do not provide banking services, nor carry on a banking business, in Australia. This research, and any access to it, is intended only for "wholesale clients" within the meaning of the Australian Corporations Act, unless otherwise agreed by Goldman Sachs. Brazil: Disclosure information in relation to CVM Instruction 483 is available at http://www.gs.com/worldwide/brazil/area/gir/index.html. Where applicable, the Brazil-registered analyst primarily responsible for the content of this research report, as defined in Article 16 of CVM Instruction 483, is the first author named at the beginning of this report, unless indicated otherwise at the end of the text. Canada: Goldman, Sachs & Co. has approved of, and agreed to take responsibility for, this research in Canada if and to the extent it relates to equity securities of Canadian issuers. Analysts may conduct site visits but are prohibited from accepting payment or reimbursement by the company of travel expenses for such visits. Hong Kong: Further information on the securities of covered companies referred to in this research may be obtained on request from Goldman Sachs (Asia) L.L.C. India: Further information on the subject company or companies referred to in this research may be obtained from Goldman Sachs (India) Securities Private Limited; Japan: See below. Korea: Further information on the subject company or companies referred to in this research may be obtained from Goldman Sachs (Asia) L.L.C., Seoul Branch. New Zealand: Goldman Sachs New Zealand Limited and its affiliates are neither "registered banks" nor "deposit takers" (as defined in the Reserve Bank of New Zealand Act 1989) in New Zealand. This research, and any access to it, is intended for "wholesale clients" (as defined in the Financial Advisers Act 2008) unless otherwise agreed by Goldman Sachs. Russia: Research reports distributed in the Russian Federation are not advertising as defined in the Russian legislation, but are information and analysis not having product promotion as their main purpose and do not provide appraisal within the meaning of the Russian legislation on appraisal activity. Singapore: Further information on the covered companies referred to in this research may be obtained from Goldman Sachs (Singapore) Pte. (Company Number: 198602165W). Taiwan: This material is for reference only and must not be reprinted without permission. Investors should carefully consider their own investment risk. Investment results are the responsibility of the individual investor. United Kingdom: Persons who would be categorized as retail clients in the United Kingdom, as such term is defined in the rules of the Financial Conduct Authority, should read this research in conjunction with prior Goldman Sachs research on the covered companies referred to herein and should refer to the risk warnings that have been sent to them by Goldman Sachs International. A copy of these risks warnings, and a glossary of certain financial terms used in this report, are available from Goldman Sachs International on request. European Union: Disclosure information in relation to Article 4 (1) (d) and Article 6 (2) of the European Commission Directive 2003/126/EC is available at http://www.gs.com/disclosures/europeanpolicy.html which states the European Policy for Managing Conflicts of Interest in Connection with Investment Research. Japan: Goldman Sachs Japan Co., Ltd. is a Financial Instrument Dealer registered with the Kanto Financial Bureau under registration number Kinsho 69, and a member of Japan Securities Dealers Association, Financial Futures Association of Japan and Type II Financial Instruments Firms Association. Sales and purchase of equities are subject to commission pre-determined with clients plus consumption tax. See company-specific disclosures as to any applicable disclosures required by Japanese stock exchanges, the Japanese Securities Dealers Association or the Japanese Securities Finance Company. Ratings, coverage groups and views and related definitions Buy (B), Neutral (N), Sell (S) -Analysts recommend stocks as Buys or Sells for inclusion on various regional Investment Lists. Being assigned a Buy or Sell on an Investment List is determined by a stock's return potential relative to its coverage group as described below. Any stock not assigned as a Buy or a Sell on an Investment List is deemed Neutral. Each regional Investment Review Committee manages various regional Investment Lists to a global guideline of 25%-35% of stocks as Buy and 10%-15% of stocks as Sell; however, the distribution of Buys and Sells in any particular coverage group may vary as determined by the regional Investment Review Committee. Regional Conviction Buy and Sell lists represent investment recommendations focused on either the size of the potential return or the likelihood of the realization of the return. Return potential represents the price differential between the current share price and the price target expected during the time horizon associated with the price target. Price targets are required for all covered stocks. The return potential, price target and associated time horizon are stated in each report adding or reiterating an Investment List membership. Goldman Sachs Global Investment Research 26 Fortnightly Thoughts Issue 70 Coverage groups and views: A list of all stocks in each coverage group is available by primary analyst, stock and coverage group at http://www.gs.com/research/hedge.html. The analyst assigns one of the following coverage views which represents the analyst's investment outlook on the coverage group relative to the group's historical fundamentals and/or valuation. Attractive (A). The investment outlook over the following 12 months is favorable relative to the coverage group's historical fundamentals and/or valuation. Neutral (N). The investment outlook over the following 12 months is neutral relative to the coverage group's historical fundamentals and/or valuation. Cautious (C). The investment outlook over the following 12 months is unfavorable relative to the coverage group's historical fundamentals and/or valuation. Not Rated (NR). The investment rating and target price have been removed pursuant to Goldman Sachs policy when Goldman Sachs is acting in an advisory capacity in a merger or strategic transaction involving this company and in certain other circumstances. Rating Suspended (RS). Goldman Sachs Research has suspended the investment rating and price target for this stock, because there is not a sufficient fundamental basis for determining, or there are legal, regulatory or policy constraints around publishing, an investment rating or target. The previous investment rating and price target, if any, are no longer in effect for this stock and should not be relied upon. Coverage Suspended (CS). Goldman Sachs has suspended coverage of this company. Not Covered (NC). Goldman Sachs does not cover this company. Not Available or Not Applicable (NA). The information is not available for display or is not applicable. Not Meaningful (NM). The information is not meaningful and is therefore excluded. Global product; distributing entities The Global Investment Research Division of Goldman Sachs produces and distributes research products for clients of Goldman Sachs on a global basis. Analysts based in Goldman Sachs offices around the world produce equity research on industries and companies, and research on macroeconomics, currencies, commodities and portfolio strategy. This research is disseminated in Australia by Goldman Sachs Australia Pty Ltd (ABN 21 006 797 897); in Brazil by Goldman Sachs do Brasil Corretora de Títulos e Valores Mobiliários S.A.; in Canada by Goldman, Sachs & Co. regarding Canadian equities and by Goldman, Sachs & Co. (all other research); in Hong Kong by Goldman Sachs (Asia) L.L.C.; in India by Goldman Sachs (India) Securities Private Ltd.; in Japan by Goldman Sachs Japan Co., Ltd.; in the Republic of Korea by Goldman Sachs (Asia) L.L.C., Seoul Branch; in New Zealand by Goldman Sachs New Zealand Limited; in Russia by OOO Goldman Sachs; in Singapore by Goldman Sachs (Singapore) Pte. (Company Number: 198602165W); and in the United States of America by Goldman, Sachs & Co. Goldman Sachs International has approved this research in connection with its distribution in the United Kingdom and European Union. European Union: Goldman Sachs International authorised by the Prudential Regulation Authority and regulated by the Financial Conduct Authority and the Prudential Regulation Authority, has approved this research in connection with its distribution in the European Union and United Kingdom; Goldman Sachs AG and Goldman Sachs International Zweigniederlassung Frankfurt, regulated by the Bundesanstalt für Finanzdienstleistungsaufsicht, may also distribute research in Germany. General disclosures This research is for our clients only. Other than disclosures relating to Goldman Sachs, this research is based on current public information that we consider reliable, but we do not represent it is accurate or complete, and it should not be relied on as such. We seek to update our research as appropriate, but various regulations may prevent us from doing so. Other than certain industry reports published on a periodic basis, the large majority of reports are published at irregular intervals as appropriate in the analyst's judgment. Goldman Sachs conducts a global full-service, integrated investment banking, investment management, and brokerage business. We have investment banking and other business relationships with a substantial percentage of the companies covered by our Global Investment Research Division. Goldman, Sachs & Co., the United States broker dealer, is a member of SIPC (http://www.sipc.org). Our salespeople, traders, and other professionals may provide oral or written market commentary or trading strategies to our clients and our proprietary trading desks that reflect opinions that are contrary to the opinions expressed in this research. Our asset management area, our proprietary trading desks and investing businesses may make investment decisions that are inconsistent with the recommendations or views expressed in this research. The analysts named in this report may have from time to time discussed with our clients, including Goldman Sachs salespersons and traders, or may discuss in this report, trading strategies that reference catalysts or events that may have a near-term impact on the market price of the equity securities discussed in this report, which impact may be directionally counter to the analyst's published price target expectations for such stocks. Any such trading strategies are distinct from and do not affect the analyst's fundamental equity rating for such stocks, which rating reflects a stock's return potential relative to its coverage group as described herein. We and our affiliates, officers, directors, and employees, excluding equity and credit analysts, will from time to time have long or short positions in, act as principal in, and buy or sell, the securities or derivatives, if any, referred to in this research. This research is not an offer to sell or the solicitation of an offer to buy any security in any jurisdiction where such an offer or solicitation would be illegal. It does not constitute a personal recommendation or take into account the particular investment objectives, financial situations, or needs of individual clients. Clients should consider whether any advice or recommendation in this research is suitable for their particular circumstances and, if appropriate, seek professional advice, including tax advice. The price and value of investments referred to in this research and the income from them may fluctuate. Past performance is not a guide to future performance, future returns are not guaranteed, and a loss of original capital may occur. Fluctuations in exchange rates could have adverse effects on the value or price of, or income derived from, certain investments. Certain transactions, including those involving futures, options, and other derivatives, give rise to substantial risk and are not suitable for all investors. Investors should review current options disclosure documents which are available from Goldman Sachs sales representatives or at http://www.theocc.com/about/publications/character-risks.jsp. Transaction costs may be significant in option strategies calling for multiple purchase and sales of options such as spreads. Supporting documentation will be supplied upon request. In producing research reports, members of the Global Investment Research Division of Goldman Sachs Australia may attend site visits and other meetings hosted by the issuers the subject of its research reports. In some instances the costs of such site visits or meetings may be met in part or in whole by the issuers concerned if Goldman Sachs Australia considers it is appropriate and reasonable in the specific circumstances relating to the site visit or meeting. All research reports are disseminated and available to all clients simultaneously through electronic publication to our internal client websites. Not all research content is redistributed to our clients or available to third-party aggregators, nor is Goldman Sachs responsible for the redistribution of our research by third party aggregators. For research or data available on a particular security, please contact your sales representative or go to http://360.gs.com. Goldman Sachs Global Investment Research 27 Fortnightly Thoughts Issue 70 Disclosure information is also available at http://www.gs.com/research/hedge.html or from Research Compliance, 200 West Street, New York, NY 10282. © 2014 Goldman Sachs. No part of this material may be (i) copied, photocopied or duplicated in any form by any means or (ii) redistributed without the prior written consent of The Goldman Sachs Group, Inc. Goldman Sachs Global Investment Research 28
© Copyright 2026 ExpyDoc