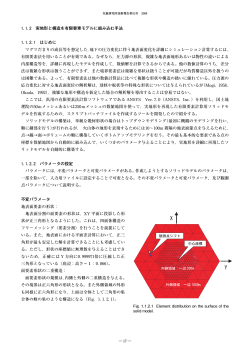
Conferment of the SSO Poster Prizes Poster pour le meilleur cas clinique Poster für die beste Fallvorstellung Cyclodialysis Cleft after Intravitreal Injection of Ranibizumab – Diagnosis and Management Böhni S., Bochmann F., Howell J., Schmid M. Augenklinik Kantonsspital Luzern Cyclodialysis Cleft after Intravitreal Injection of Ranibizumab – Diagnosis and Management Böhni SC, Howell JP, Bochmann F, Schmid MK FINANCIAL INTERESTS / GRANTS: Dr. Böhni’s work was funded via an unrestricted educational grant by Novartis Switzerland AG BACKGROUND Since the introduction of anti-vascular endothelial growth factor (anti-VEGF) for treatment of choroidal neovascularisation, the number of intravitreal injections (IVI) via pars plana has increased tremendously. Complications of intravitreal injections are rare, but potentially sight threatening.1 HISTORY AND SIGNS A 57-year old female underwent her 8 th IVI of Ranibizumab for treatment of myopic choroidal neoavascularisation. The following bday, the patient presented with deteriorated visual acuity and an IOP of 2mmHg. Gonioscopy disclosed a cyclodialysis cleft in the inferonasal quadrant (Figure 1). UBM confirmed the diagnosis and revealed a splitting of the ciliary body (Figure 2). e THERAPY AND OUTCOME Surgical cleft repair was conducted by dissection of a limbal based scleral lamella and reattachment of the ciliary body with a 10/0 polypropylen suture. The sutures were placed transcamerally through the pupil and the ciliary sulcus (Figure 3). As expected, the IOP rose to a very high level on the first postoperative day, which was, however, manageable with topical and systemic aqueous suppressants. Two weeks postinterventionally, the IOP reached normal levels without any further treatment. The symptoms disappeared and visual acuity recovered. c f Figure 3 Intraoperative picture of the transchamber sutures, showing the straight needle passing under the iris, leaving the eye via the ciliary sulcus. Figure 1 Gonioscopy showing the inferonasal cyclodialysis cleft CONCLUSIONS A cyclodialysis cleft is a rare complication of an IVI and should be suspected in cases with persisting low intraocular pressure. A careful planning of the injection site may help to prevent this complication.2 While for diagnostic measures, gonioscopy and ultrasound biomicroscopy are the investigations of choice3, from a therapeutic point of view the reattachment of the ciliary body using transchamber sutures has shown to be effective. REFERENCES Figure 2 UBM performed one day after the IVI: Splitting of the ciliary body (Arrow) at eight o‘clock 1 Shima C, Sakaguchi H, Gomi F, Kamei M, Ikuno Y, Sawa M, Tsujikawa M, Kusaka S, Tano Y (2008) Complications in patients after intravitreal injection of bevacizumab. Acta Ophthalmol 86: 372-376 2 Dahrab MM, Laroch GR (2011) Error of calibration in ophthalmic calipers: a source of significant clinical errors. Can J Ophthalmol 46: 510-512 3 Ioannidis AS, Barton K (2010) Cyclodialysis cleft: causes and repair. Curr Opin Ophthalmol 21: 150-154 Poster pour le meilleur cas clinique Poster für die beste Fallvorstellung Autologous internal limiting membrane (ILM) recycling to close very large refractory macular holes Wolfensberger T. Jules Gonin Eye Hospital, University of Lausanne Autologous internal limiting membrane (ILM) recycling to close very large refractory macular holes Thomas J. Wolfensberger Hôpital ophtalmique Jules-Gonin, Lausanne Background: • Large macular holes refractory to repeated macular surgery with ILM peeling are very difficult to close. • Re-peeling of some epiretinal tissue or massaging of the macular hole rim may be done, although its benefits are debated and it may harm the residual photoreceptors. Case Report: • 62 year old female patient, previously operated on elsewhere twice without success for a macular hole by vitrectomy, ILM peeling, ILM re-peeling and gas tamponnade • Patient referred with very large stage IV macular hole of 857 µm. Best-corrected visual acuity 0.05p. Pre-op Post-op VA: 0.05 VA: 0.2p 857 µm Fig 1. Pre-operative OCT with stage IV macular hole (diameter of 857 µm) with marked edematous changes in the outer and inner retinal layers of the macular hole rim. Fig 2. Post-operative OCT showing a completely closed macular hole with disappearance of the edematous changes Therapy and Outcome: • 23g vitrectomy with free autologous transplant of ILM taken from the temporal periphery of the macula and inserted into macular hole before 23% SF6 gas tamponnade. Fig 3. Pre-operative situation with denuded ILM peeled during previous surgeries ILM Retina Bruch Fig 4 A piece of fresh ILM is peeled outside the previously peeled area Fig 5. The ILM transplant is transferred into the macular hole to create a plug • Follow-up: Complete closure of the macular hole at 10 days, visual acuity increase to 0.2p at 8 months. [email protected] www.ophtalmique.ch ILM Retina Bruch Conclusion: Autologous ILM recycling to close large macular holes refractory to surgical treatment is a simple and elegant technique in situations where no other manœuvre is likely to achieve hole closure. References: Valldeperas X, Wong D. Is it worth reoperating on macular holes? Ophthalmology. 2008 Jan;115(1):158-63. D’Souza MJ et al. Re-operation of idiopathic full-thickness macular holes after initial surgery with ILM peel. Br J Ophthal. 2011 Nov;95(11):1564-7. Morizane Y, et al. Autologous transplantation of the ILM for refractory macular holes. Am J Ophthalmol. 2014 Apr;157(4):861-869 Poster pour la meilleure étude Poster für die beste Studie Measurement of optic nerve sheath diameter by CT, MRI and ultrasound Giger Tobler C., Eisenack J., Holzmann D., Pangalu A., Sturm V., Killer H., Landau K., Jaggi G. Augenklinik USZ, Zürich, ORL-Klinik Universitätsspital, Zürich, Institut für Neuroradiologie, Zürich, Kantonsspital Augenklinik, St. Gallen, Kantonsspital Augenklinik, Aarau Measurement of optic nerve sheath diameter by CT, MRI and ultrasound C. Giger Tobler 1, J. Eisenack 1, D. Holzmann 2, A. Pangalu 3, V. Sturm 4, H.E. Killer 5, K. Landau 1, G.P. Jaggi 1 UniversityHospital Zurich 1) University Hospital Zurich, Department of Ophthalmology, Zurich, Switzerland 2) University Hospital Zurich, Department of ENL, Zurich, Switzerland 3) University Hospital Zurich, Department of Neuroradiology, Zurich, Switzerland 4) Cantonal Hospital of St.Gallen, Department of Ophthalmology, St.Gallen, Switzerland 5) Cantonal Hospital of Aarau, Departement of Ophthalmolgy, Aarau, Switzerland No financial interests Background Quantification of the optic nerve sheath diameter (ONSD) is promising for detection of altered intracranial pressure [1-4]. Until now the comparability of current methods is unclear. The objective of this study was to assess the relationship between ONSD, as measured using CT, MRI and transbulbar sonography (US) in optic nerves of subjects with presumably normal intracranial pressure and to find correlations and/or significant discrepancies between the different imaging methods [5-6]. Methods 15 patients (60.8 [y] ±16.73 SD; 7 females) with paranasal sinuses pathology without known optic nerve pathology and existing CT and MRI underwent ONSD measurements by US (Quantel Medical), as well as a complete ophthalmological examination. US-, CT-, and MRI-derived maximal ONSD values 3mm behind the globe were compared by Bland-Altman plot [7]. Correlation analyses were performed using Spearman-Rho’s correlation coefficient (ρ). Statistics were performed using SPSS Version 22.0.0.0 (PASW/SPSS IBM Corporation , New York, NY, USA). Fig 1 Fig 1: Box-Plot of optic nerve sheath diameter values measured by CT (blue bar), MRI (green bar), transbulbar sonography (yellow bar). r = right eye; l = left eye. Fig 2 Fig 2: Comparability within CT and MRI by Bland Altman plot. Continuous line depicts the mean of difference (-0.14[mm]); dashed lines denote limits of agreement (+1.96 SD = 1.08[mm]; -1.96 SD = -1.37). Right eye (green dot); left eye (red dot). Fig 4 Fig 3 Fig 3: Comparability within CT and transbulbar sonography by Bland Altman plot. Continuous line depicts the mean of difference (-1.01[mm]); dashed lines denote limits of agreement (+1.96 SD = 0.73[mm]; -1.96 SD = -2.76). Right eye (green dot); left eye (red dot) Fig 4: Comparability within MRI and transbulbar sonography by Bland Altman plot. Continuous line depicts the mean of difference (-0.87[mm]); dashed lines denote limits of agreement (+1.96 SD = 0.98[mm]; -1.96 SD = -2.73). Right eye (green dot); left eye (red dot) Results ONSD measured (n=30) by US (mean 6.2 [mm]±0.84SD; range 4.6 - 8.3) were significantly (p<0.01) higher than ONSD in CT (5.2±1.11; range 3.4 - 7.2 ) or MRI (5.3±1.14; range 3.6 - 8.0). [Fig 1] There was no significant (P=0.24) difference but good correlation (ρ=0.854, p<0.01) between ONSD measured in CT and MRI. Those of US and CT (ρ=0.662, p<0.01) and US and MRI (ρ=0.615, p<0.01) showed a modest but significant correlation. The Bland Altman analysis revealed a comparability within the methods. [Fig 2-4] No correlation between ONSD and age as well as ONSD and gender could be seen using multivariate analysis. Conclusion The comparability of ONSD measurements between CT, MRI and US seems to be given. Only a modestly significant correlation was found between US and CT and US and MRI. In this study the measured ONSD by US showed a slightly higher value than ONSD measured by CT or MRI. Furthermore ONSD by US reported in other studies [5-6] were slightly smaller than in this study. Values for MRI were completely in accordance with existing studies [6,8]. To the best of our knowledge this study is the first to compare ONSD measurements in a group of subjects in whom all three imaging studies e.g. CT, MRI and US were used simultanously. References: 1. Soldatos T, Chatzimichail K, Papathanasiou M, Gouliamos A. Optic nerve sonography: a new window for the non-invasive evaluation of intracranial pressure in brain injury. Emerg Med J 2009;26:630-4. 2. Watanabe A, Kinouchi H, Horikoshi T, Uchida M, Ishigame K. Effect of intracranial pressure on the diameter of the optic nerve sheath. J Neurosurg 2008;109:255-8. 3. Sutherland AI, Morris DS, Owen CG, Bron AJ, Roach RC. Optic nerve sheath diameter, intracranial pressure and acute mountain sickness on Mount Everest: a longitudinal cohort study. Br J Sports Med 2008;42:183-8. 4. Kimberly HH, Noble VE. Using MRI of the optic nerve sheath to detect elevated intracranial pressure. Crit Care 2008;12:181. 5. Maude RR, Hossain MA, Hassan MU, Osbourne S, Sayeed KLA, Karim MR, et al. Transorbital Sonographic Evaluation of Normal Optic Nerve Sheath Diameter in Healthy Volunteers in Bangladesh. PLoS ONE 2013;8(12) 6. Bäuerle J, Schuchardt F, Schroeder L, Egger K, Weigel M, Harloff A. Reproducibility and accuracy of optic nerve sheath diameter assessment using ultrasound compared to magnetic resonance imaging. BMC Neurology 2013;13:187 7. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;307-10. 8. Weigel M, Lagrèze WA, Lazzaro A, Henning J, Bley TA. Fast and quantitative high-resolution magnetic resonance imaging of the optic nerve at 3.0 tesla. Invest Radiol 2006, 41:83-86 Poster pour la meilleure recherche fondamentale Poster für die beste Grundlagenforschung Compound heterozygous VSX2 mutations causing bilateral anophthalmia in a consanguineous family Jakobsson C., Youssef M., El Shakankiri N., Marzouk I., Bayoumi N., Munier F., Schorderet D., Abou Zeid H. Jules Gonin Eye Hospital, University of Lausanne, Dpt of Genetic, Univerisity EG-Alexandria, Dpt of Ophthalmology, University EG-Alexandria, HOJG, Lausanne, IRO, Sion Compound heterozygous VSX2 mutations causing bilateral anophthalmia in a consanguineous family. C.Jakobsson1,2, Mohamed A. Youssef3, Iman Marzouk3, Nihal ElShakankiri4, Nader Bayoumi4, F.L. Munier1,2, D.F. Schorderet1,2,5 and H. Abouzeid1 1 IRO-Institute for Research in Ophthalmology, Sion; 2Jules-Gonin Eye Hospital, Fondation Asile des Aveugles, Department of ophthalmology, University of Lausanne, Lausanne; 3Genetics Unit, Department of Pediatrics, University of Alexandria, Alexandria, Egypt; 4Department of Ophthalmology, University of Alexandria, Alexandria, Egypt; 5EPFL-Ecole polytechnique fédérale de Lausanne, Lausanne PURPOSE: To report the clinical and genetic study of a child with bilateral anophthalmia. BACKGROUND: • Anophthalmia is found in 1 of 5 000 to 10 000 individuals. • More than 60% of patients do not receive a molecular . diagnosis. • The transcription factor SOX2 is the main causing gene for anophthalmia/microphtalmia (A/M) and is mutated in 10-20% of patients. MOLECULAR RESULTS : • Sequencing analysis revealed a hemizygous exon 2 mutation in the VSX2 gene, [c.422delA; p.N141Ifs*19] in the affected child. • This mutation was heterozygous in his unaffected father and absent in his mother, suggesting the presence of a deletion that included at least exon 2 of VSX2 in the mother. • The novel mutation was not detected in 96 controls from North Africa. METHODS: • One patient, a 14-year-old boy, with clinical anophthalmia and first-degree relatives from a consanguineous family of Egyptian origin underwent full ophthalmic, general and neurological examination, as well as blood drawing. • Genomic DNA was extracted from peripheral blood, and genetic analysis was performed in the parents and the child. • Direct sequencing, by Sanger method, of all 5 exons of VSX2 was performed after PCR amplification. Patient Mother Father FIGURE 1 Pedigree of the consanguineous Egyptian family." Squares indicate males, circles females. The filled symbol indicates the affected 14-year-old boy with bilateral anophthalmia and the double line indicates consanguinity." CLINICAL RESULTS : DISCUSSION: • In this study, we identified new compound VSX2 deletions causing bilateral anophthalmia: c.422delA and exon 2 deletion. • The novel mutation observed in this study and its absence in 96 healthy individuals from North Africa, strongly suggest that this change disrupts VSX2 function. • To date, only eight different homozygous mutations in VSX2 have been associated to A/M in eleven consanguineous families descending from Arabic countries or neighbouring regions. • VSX2 is an important gene for embryogenesis, proliferation, differentiation and fate of the developing cell. Evidence shows that a restricted expression of VSX2 correspond to a mice characterized by an abnormal ocular development. CONCLUSIONS: [email protected] www.ophtalmique.ch • In addition to bilateral anophthalmia, arachnodactyly and high arched palate was observed in the affected patient. He presented normal psychomotor development and was normal for length, weight and head circumference. • Parents were healthy. FIGURE 4: Sanger sequencing of VSX2 exon 2. Patient shows hemizygous deletion of nucleotide A at position 422. Mother has a wild-type sequence while father is heterozygous for the deletion. As the mother does not show a heterozygous sequence, she must have a complete deletion of at least exon 2 of VSX2. • A compound heterozygous VSX2 mutation associated with FIGURE 2 anophthalmia was identified in a patient from a Photographes of the 14-year-old boy affected by bilateral consanguineous family of Egyptian origin. This study anophthalmia. Note the complete absence of both eyes, the large expands the number of mutations causing severe A/M and eyebrows and low insertion on the superior eyelid. the causality of VSX2. FIGURE 3 Note the arachonodactyly of the feet • Functional consequences of the reported changes still need to be characterized, as well as the percentage of anophthalmia caused by mutations in the VSX2. • This family also shows that despite consanguinity, heterozygous mutations can also occur and one should not restrict the molecular analysis to homozygous mutations.
© Copyright 2026 ExpyDoc