Expy
Doc
Explore Categories
Log in
Create new account
No category
3rd Qtr. 2014 Fee Schedule Worksheet.xlsx
Download
Report
POB Overview PMM Mtg 7-10 Final.pptx
Refrigerator Temperature Log
Michigan Tigers Futbol Club
貳、服務類用詞
Futbol Club of Santa Rosa 2014-2015
Current Price Grid
2014-2015 学生报名表/REGISTRATION FORM - (LISOC)
Prime Pac™ PRRS+ - Merck Animal Health
Entry - Oregon Horse Center
here. - Ruyton Girls School
here - Hollard Broker Zone
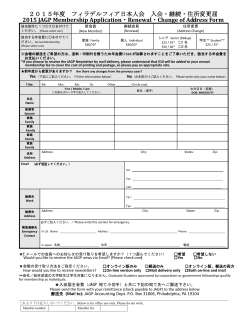
2015年度 フィラデルフィア日本人会 入会・継続・住所変更届 2015
© Copyright 2026 ExpyDoc
About ExpyDoc
DMCA / GDPR
Report