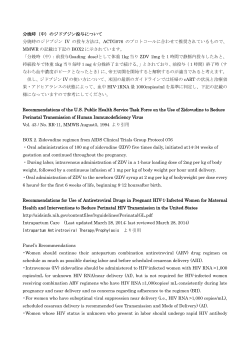
重症血友病 A 男児を対象にした完全な定期補充療法達成の方法: 各種レジメンならびに早期出血および静脈アクセスに及ぼす影響 How to achieve full prophylaxis in young boys with severe haemophilia A: different regimens and their effect on early bleeding and venous access A. Nijdam, K. Kurnik, R. Liesner, R. Ljung, B. Nolan, P. Petrini and K. Fischer on behalf of the PedNet Study Group Van Creveldkliniek, University Medical Center, Utrecht, The Netherlands; Dr. von Haunersches Children ’ s Hospital, University of Munich, Munich, Germany; Haemophilia Center, Department of Haematology Great Ormond Street Hospital for Children, London, UK; Department of Clinical Sciences Lund – Paediatrics and Malmö Haemostasis & Thrombosis Centre, Lund University, Skåne University Hospital, Malmö, Sweden; Department of Haematology Oncology, Our Lady ’ s Children ’ s Hospital, Crumlin, Dublin, Ireland; Paediatric Department of Coagulation Disorders, Karolinska University Hospital, Stockholm, Sweden; and Julius Center for Health Sciences and Primary Care University Medical Center, Utrecht, The Netherlands 要 約:早期の定期補充療法促進のため,定期補充 の 36%)。(iii)週 1 ~ 2 回から開始し,出血表現 療法を週 1 回の輸注により開始し,これを漸増させ 型(phenotype )に応じて頻度を増加させ,3 歳以 るレジメンが導入された。初期レジメンの選択は, 降週 3 回以上に到達(施設の 38%,患者の 46%)。 転帰に影響を及ぼす可能性がある。本研究は,初期 定期補充療法開始年齢の中央値は,full および asap の定期補充療法レジメンを分類し,その短期転帰に レジメンでは 1.2 歳であったのに対し,phenotype つ い て 比 較 す る こ と を 目 的 と し た。「European レジメンでは 1.8 歳であった。関節内出血の完全予 Paediatric Network for Haemophilia Management」 防に最も効果を示したのは full レジメンであった (PedNet)レジストリから,インヒビターを保有し (full 32% に対して,asap 27%,phenotype 8%)。 ない重症血友病 A 患者で,2000 ~ 2012 年に出生 一方,full レジメンは CVAD の使用が最も多いと した定期補充療法施行患者のデータを入手した。治 いう損失を生じた(full 88% に対して,asap 34%, 療施設は,初期の定期補充療法の輸注頻度および週 phenotype 22%)。今回確認された 3 種類の定期補 充療法レジメンは,早期の出血および CVAD の使 3 回以上の輸注に到達した年齢に基づいて分類され た。出血および中心静脈アクセスデバイス(CVAD) 用に及ぼす影響に違いがあった。今回の分類は,最 の使用状況について,4 歳の時点で比較を行った。 適な定期補充療法レジメンの確立に向けた最初のス 患者 363 名・21 施設において,次の 3 種類のレジ テップである。 メンが確認された。 (i)週 3 回以上の定期補充療法 の輸注を 3 歳になる前に開始〔完全(full ):施設 Keywords: bleeding , central venous catheters , 患者の 18%〕。 (ii) 週 1 ~ 2 回から開始し, children , haemophilia A , prophylaxis , step-up の 19%, 可能な限り速やか(asap )に頻度を増加させ,3 歳 regimen になる前に週 3 回以上に到達(施設の 43%,患者 the asap regimen, the majority of patients started patient on once weekly prophylaxis at 3.8 years of prophylaxis before the onset of joint bleeding, age who did not follow the regular protocol in a cenwhereas patients on the full and phenotype regimens tre using the asap regimen. bleed prompted STRATEGIES FOR STARTING EARLYThis PROPHYLAXIS 5 FOR START experienced a median of one joint bleed before startimmediate stepping up to infusions every otherSTRATEGIES day. ing prophylaxis (P < 0.01). Starting prophylaxis Overall, the proportion of intracranial bleeds and the (a) Discussion Prophylaxis ≥3x/week (a) at which they occurred were similar across the before the third joint bleed was achieved in 89% of age Discussion Prophylaxis ≥3x/week Principal findings Table 1. Patient and treatment characteristics according to prophylactic strategies. Principal findings *Due to clinical circumstances not all patients in a centre started prophylaxis according to the local regimen. Three different regi identified in Eu ≥39 week1 before prophylaxis with and stepping up t 3 years (as soon as to patient’s bleeding Full and asap reg treatment intensity regimen reached ≥3 much less CVADs phenotype regimen experienced two ad but needed fewer C Three different regimens for starting prophylaxis were FULL ASAP PHENOTYPE centres: identified in European starting with Prophylactic strategy Full prophylaxis As soon as possible1 According to bleeding P-value across strategies ≥39 week before the age of 3 years (full), starting Number of centres (%) 4 (19) 9 (43) 8 (38) prophylaxis with lower frequencies (1–29– week1) Number of patients on prophylaxis (%) 66 (18) 130 (36) 167 (46) – and stepping up to ≥39 week1 before the Age at 1st treatment 0.8 (0.3–1.1) 0.9 (0.6–1.1) 0.8 (0.5–1.1) 0.49age of 3 years (as soon as possible: asap) or later (according At starting prophylaxis Age 1.3 (0.9–1.8) 1.2to(0.9–1.5) 1.7phenotype). (1.2–2.6) <0.01 patient’s bleeding Frequency 19 week1 9%* 49% 55% <0.01 Full and asap regimens showed similar bleeding and Frequency 29 week1 8%* 35% 31% <0.01 treatment intensity. However, patients on<0.01 the asap Frequency ≥39 week1 83% 16%* 14%* Infusion dose in IU kg1 52 (40–87) 46 (28–51) reached ≥39 41 (32–48) and used regimen week1 6 months later<0.01 At reaching ≥39 week1 much less CVADs (88% vs. 34%). Patients on the Age 1.3 (0.9–1.8) 1.8 (1.2–3.1) 3.9 (2.3–6.0) <0.01 last and regimen1.6 (0.2–3.8) reached ≥39 week1 <0.01 Time to reach ≥39 week1 since starting 0.0 (0.0–0.0) 0.4phenotype (0.1–1.9) 1 experienced two additional 4 years, 51 (39–88) 34 (24–47) 29 (23–37) joint bleeds at age <0.01 Infusion dose in IU kg Values are numbers, proportions, medians (IQR) and P-values across strategies. but needed fewer CVADs (22%) and infusions. STRATEGIES FOR STARTING EARLY PROPHYLAXIS (b) Haemophilia (2014), 1--7 (a) Internal and external validity 5 © 2014 John Wiley & Sons Ltd (b) Analyses were based on the high-quality detailed dataDiscussion base from the repeatedly checked and monitored PedNet registry; data on EDs were missing in 4% only Principal [15]. Start findings of prophylaxis was easy to assess, as it generally thefor firststarting 75 EDsprophylaxis that were docuThree occurred different within regimens were mented detail. Follow-upcentres: of outcome datawith on identifiedin in European starting 1 bleeding, of infusions clotting factor conbefore the age ofand 3 years (full), starting ≥39 weeknumber 1 sumption waswith limited to age 4 years, as it was avail) prophylaxis lower frequencies (1–29 week 1 and by then most able for the majority of patients before the age of and stepping up to ≥39 week 1 . patients hadsoon reached prophylaxis ≥39 3 years (as as possible: asap) or week later (according The classification of regimens at centre level is an to patient’s bleeding phenotype). essential part of regimens this study. Selection biasbleeding (confoundFull and asap showed similar and ing by indication) wasHowever, avoided by analysing treatment intensity. patients on strategies the asap 1 cohorts of patients with at centre reached level, including full 6 months later and used regimen ≥39 week different phenotypes. much less CVADs (88% vs. 34%). Patients on the 1 The classification of prophylactic regimens last was and phenotype regimen reached ≥39 week based on published data showing the strong experienced two additional joint bleeds at ageindepen4 years, dent effect of age CVADs at starting prophylaxis on outcome but needed fewer (22%) and infusions. [4,19]. Differences between centres, other than prophylaxis start regimen, may affect outcome, but are Internal to and Fig. 3. Cumulative incidence of (a) reaching ≥3 times week1 and (b) cenunlikely beexternal the mainvalidity driver of differences between (b) Fig. 3. Cumulative incidence of (a) reaching ≥3 times week1 and (b) central venous access device (CVAD) use according to regimen. The Kaplan– regimens. Analyses were device based(CVAD) on the detailed datatral venous access usehigh-quality according to regimen. The Kaplan– Meier one minus survival function estimates cumulative incidences, Meier one minus survival estimates cumulative incidences, Thefrom classification wasfunction verified with treating phyadjusted for inhibitor development and incomplete follow-up. base the repeatedly checked andthe monitored Ped6 A. NIJDAM et al. adjusted for development and incomplete follow-up. have forsicians at inhibitor the data centres. centres Net registry; on Although EDs werefew missing in 4% only three prophylactic regimens. No other potentially mal all treatingwas physicians agreed as with the [15].protocols, Start of prophylaxis easy to assess, it genTable 2. Bleeding and treatment up to age 4 years according to prophylactic strategy. three occurred prophylactic regimens. potentially life-threatening bleeds were observed in the cohort. classification of within their prophylactic strategy. erally the first 75No EDsother that were docuFULL ASAP PHENOTYPE life-threatening bleeds were observed the cohort. These datadetail. represent treatment inincountries mented in Follow-up of outcome datawith on Prophylactic strategy Full prophylaxis As soon as possible According to bleeding good access to treatment andand medical care and no bleeding, number of infusions clotting factor conNumber of patients 66 130 167 P-value across strategies Factor administrations and consumption restrictions in clotting factor consumption It is sumption was limited to age consumption 4 years, as it only. was availFactor administrations and Before starting prophylaxis AtCumulative the age number of 4 years, infulikely thatthe prophylactic treatment including able0 (0–1) for majority1 of patients strategies, and by <0.01 then most of joint the bleedscumulative number 1of (0–1) (1–3) At65% the age 4ofyears, the cumulative number 1 Without joint bleeds 20% <0.01 sions received was close to 400 for both the 42% full and the introduction prophylaxis, are≥39 different elsewhere. . of infupatients hadofreached prophylaxis week sions received was close to 400 for both the fullis and Number of ICHs (% of all patients) 8 (10) 7 (5) 10 (5) 0.22 asap regimens, whereas significantly lower on the phenoThe classification of regimens at centre level an At 4 years of age asap regimens, whereas significantly lower on(confoundthe phenotype regimen (223; P < 0.01). Concurrently, the total essential part of this study. Selection bias Cumulative number of joint bleeds 1 (0–2) 1 (1–3) 3 (1–5) <0.01 Other studies type (223;was P8% <avoided 0.01). Concurrently, the total clotting consumption at age 4 years was32% around Without factor joint bleeds 27% ing byregimen indication) by analysing<0.01 strategies clotting factor age 4 years was around Cumulative of infusions 360 (186–500) 402 (275–496) (119–343) <0.01 174 000 IUnumber on the full and asap regimens and about Most information on223 effective prophylaxis is available at centre level, consumption including fullatcohorts of patients with Cumulative clotting factor consumption (in 1000 IU) 177 (72–340) 172 000 (109–238) 90 (53–149) <0.01 174 IU on the full and asap regimens and about half of that on the phenotype regimen (P < 0.01). on starting prophylaxis before age 3 years or before different phenotypes. Values are numbers, proportions, medians (IQR) and P-values across strategies. half of that on the phenotype regimen (P < 0.01). The classification of prophylactic regimens was ICHs, intracranial haemorrhages. based on published data showingHaemophilia the strong(2014), indepen© 2014 John Wiley & Sons Ltd 1--7 © 2014 John of Wiley Ltd dent effect age&atSons starting prophylaxis on outcome Haemophilia (2014), 1–7 DOI: 10.1111/hae.12613 [4,19]. Differences between centres, other than protheWiley third&joint to ≥39 week1 after implantation, avoiding CVAD © 2014 John Sons bleed Ltd [4,19]. This is reflected in current phylaxis start regimen, may affect outcome, but are 1 clinical practice: all three regimens generally use was not the only reason to start at lower frequenhttp://onlinelibrary.wiley.com/doi/10.1111/hae.12613/abstract Fig. 3. Cumulative incidence of (a) reaching ≥3 times week andstarted (b) cenunlikely to be the main driver of differences between tral venous accessbefore device (CVAD) use of according to regimen. The Kaplan– prophylaxis the age 3 years and before the cies. Introducing prophylaxis at lower frequencies is regimens. Meier one survival function estimates cumulative incidences, 本誌の日本語訳は原著者の許可を得てワイリー・パブリッシング・ジャパンが作成しています。 third jointminus bleed. However, to improve prophylactic also thought to increase patients’ and parents’ accepThe classification was verified with the treating phyadjusted for inhibitor development and incomplete follow-up. 無断複製・転載・修正は著作権法により禁じられています。 treatment, it is important to study outcome of differtance of treatment [25]. sicians at the centres. Although few centres have for詳しくは「ヘモフィリアステーション」 をご覧ください。 ent regimens beyond the initiation phase of prophythree prophylactic regimens. No other potentially mal protocols, all treating physicians agreed with the http://www.hemophilia-st.jp/medical/ laxis. life-threatening bleeds were observed in the cohort. classification of their prophylactic strategy. Clinical implications The full regimen can be compared to the randomThese data represent treatment in countries with To move towards more optimal treatment strategies, ized trials of the Joint Outcome Study (n = 32) [20] good access to treatment and medical care and no Factor it is important to assess regimens used in clinical pracand theadministrations ESPRIT study and (n =consumption 21) [21] which started restrictions in clotting factor consumption only. It is tice. The data presented provide extensive experience prophylaxis with 3–3.59 week1. However, as they At the age of 4 years, the cumulative number of infulikely that prophylactic treatment strategies, including started prophylaxis at older ages than those on the in starting early prophylaxis for severe haemophilia A. sions received was close to 400 for both the full and the introduction of prophylaxis, are different elsewhere. Comparing short-term benefits and burden across regifull regimen in this study, outcome cannot be comasap regimens, whereas significantly lower on the phenomens, the asap regimen seems to provide the best of pared. type regimen (223; P < 0.01). Concurrently, the total Prophylaxis ≥3x/week Internal and extern Analyses were base base from the repe Net registry; data [15]. Start of proph erally occurred with mented in detail. bleeding, number o sumption was limit able for the major patients had reache The classification essential part of th ing by indication) w at centre level, incl different phenotype The classificatio based on published dent effect of age a [4,19]. Differences phylaxis start regim unlikely to be the regimens. The classification sicians at the centr mal protocols, all t classification of the These data repr good access to tre restrictions in clott likely that prophyla the introduction of Other studies Most information o on starting prophy
© Copyright 2026 ExpyDoc