J C E M
A d v a n c e s
i n
G e n e t i c s — E n d o c r i n e
O N L I N E
R e s e a r c h
Androgen Receptor CAG Repeat Length Is Associated
With Body Fat and Serum SHBG in Boys: A Prospective
Cohort Study
Annette Mouritsen, Casper P. Hagen, Kaspar Sørensen, Lise Aksglaede,
Mikkel G. Mieritz, Katharina M. Main, Kristian Almstrup, Ewa Rajpert-De Meyts,
and Anders Juul
Department of Growth and Reproduction, Rigshospitalet, Faculty of Health Sciences, University of
Copenhagen, 2100 Copenhagen, Denmark
Background: Longer androgen receptor gene CAG trinucleotide repeats, AR (CAG)n, have been
associated with reduced sensitivity of the androgen receptor (AR) in vitro as well as in humans.
Furthermore, short AR (CAG)n have been associated with premature adrenarche.
CD
R
Objective: The aim of the study was to evaluate associations between the AR (CAG)n polymorphism
and development of pubic hair, levels of androgens, and body fat content in healthy boys.
da
p
or
Methods: A longitudinal study of 78 healthy boys (age 6.2–12.4 years at inclusion) from the COPENHAGEN Puberty Study was conducted with clinical examinations and blood samples drawn
every 6 months. The AR (CAG)n length was established by direct DNA sequencing and reproductive
hormones were measured in serum by standardized analyses.
pi
aa
ut
or
iza
Results: Median AR (CAG)n length was 22 (range, 17–30). Before puberty (at 10 years of age), boys
with long CAG repeats (CAG ⱖ24) had lower levels of SHBG (88 vs 125 nmol/L) (P ⬍ .05) and a
nonsignificant trend toward higher median skinfold thickness (41 vs 31 mm) (P ⫽ .06) compared
with boys with an average number of CAG repeats (CAG 21–23). In contrast, the inverse association
was observed at puberty (at 12 years of age) in boys with short CAG repeats (CAG 17–20) (P ⬍ .05).
Serum levels of LH and testosterone (at 12 years) were significantly higher in boys with long CAG
repeats compared with boys with an average number of CAG repeats (P ⫽ .05).
Co
Conclusion: The observed associations between AR (CAG)n and peripubertal fat accumulation and
serum SHBG concentrations indicate that this genetic polymorphism may influence the androgendependent fine-tuning of metabolic and reproductive factors at a young age. (J Clin Endocrinol
Metab 98: E605–E609, 2013)
ndrogens mediate their effects primarily through activation of the androgen receptor (AR). The X-chromosomal AR contains a highly polymorphic region with
variable number of CAG repeats, (CAG)n, which encodes
a polyglutamine tract in the N-terminal transactivation
domain of the receptor (1). A negative linear association
between AR sensitivity and CAG repeat length has been
proposed based on the presentation of partial androgen
resistance in men with spinobulbar dystrophy (Kennedy
syndrome) caused by AR CAG repeat lengths greater than
A
40 (2), supported by 2 in vitro studies (3, 4). Subsequently,
numerous epidemiological studies have associated longer
AR (CAG)n, with disorders linked to reduced androgen
activity, eg, male subfertility (5). However, whether the
association between (CAG)n and androgen receptor activity is linear seems to be contentious (6, 7).
A recent in vitro study investigated transcriptional activity of AR carrying different (CAG)n within the normal
range and observed reduced AR activity in cells transfected with AR containing both shorter (16) and longer
ISSN Print 0021-972X ISSN Online 1945-7197
Printed in U.S.A.
Copyright © 2013 by The Endocrine Society
doi: 10.1210/jc.2012-3778 Received November 1, 2012. Accepted December 28, 2012.
First Published Online February 7, 2013
Abbreviations: AR, androgen receptor; BMI, body mass index; CV, coefficient of variation;
DHEAS, dehydroepiandrosterone; TV, testicular volume.
J Clin Endocrinol Metab, March 2013, 98(3):E605–E609
jcem.endojournals.org
25/04/2014
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 24 April 2014. at 14:37 For personal use only. No other uses without permission. . All rights reserved.
E605
E606
Mouritsen et al
Androgen Receptor CAG Repeats and Body Fat in Boys
J Clin Endocrinol Metab, March 2013, 98(3):E605–E609
ation (CVs) were less than 5% in both gonadotropin assays.
Testosterone levels were measured with the DPC Coat-A-Count
radioimmunoassay kit (Diagnostic Products, Los Angeles, California) with detection limit of 0.23 nmol/L and the intra- and
interassay CVs were 7.6% and 8.6%, respectively. DHEAS and
androstenedione levels were measured by specific solid-phase,
competitive chemiluminescent enzyme immunoassays (Immulite
2000; Siemens, Erlanger, Germany) with detection limits of 0.41
mol/L and 1.04 nmol/L, respectively. The intra- and interassay
CVs were 6.3% to 7.1% and 7.8% to 10.2% and 7.1% to 10.8%
and 11.0% to 14.9%, respectively.
(28) CAG repeats compared with the medium-length (22)
CAG allele, suggesting that the association between repeat
length and AR activity is nonlinear (8). Short AR (CAG)n
have been associated with premature adrenarche (9), and
longer AR (CAG)n have been associated with earlier pubertal growth spurts in boys (10). However, it is not
known whether the length of the AR (CAG)n is associated
with age at pubertal onset and body fat accumulation in
healthy boys.
In this prospective cohort study of healthy boys followed
during pubertal transition, we aimed to evaluate whether
short and long AR (CAG)n, respectively, were associated
with clinical and biochemical markers of androgen activity,
ie, pubertal onset (gonadarche and pubarche), fat accumulation, and circulating testosterone, LH, SHBG, dehydroepiandrosterone (DHEAS), and ⌬4-androstenedione.
Genotyping
R
Molecular analysis of the AR gene polymorphism was performed using genomic DNA purified from peripheral blood samples. The CAG repeat⫺containing part of exon 1 of the AR gene
was amplified by nested PCR using 2 sets of primers in a single
reaction, and the CAG repeat number was established by direct
sequencing. The method has been validated in our laboratory in a
series of 116 fertile healthy Danish men, who had a mean of 21.8
and a median of 21 (range 14 –33) CAG repeats (6). The median
(P ⫽ .05) and distribution (P ⫽ .74) did not differ from the current
study.
CD
Subjects and Methods
da
p
Statistical analysis
Data for CAG distribution are presented as median and
range; all other data are presented as median and 25th and 75th
percentiles. Nonparametric Mann-Whitney test was used to
compare boys with short or long CAG repeats with boys with
medium CAG repeat length according to hormone levels, body
composition (body mass index [BMI] and sum of 4 skinfolds) and
hormone levels. Pearson correlation was used to estimate correlations between CAG length and SHBG or body fat. Comparisons of distributions between groups were performed by the
Levene test. To counteract the problem of multiple comparisons,
we could have used the Bonferroni correction. The method is
conservative and assumes that all 3 comparisons between the 3
groups in the study are conducted. Because only 2 comparisons
between groups (low vs medium and high vs medium) were conducted, our P values are not corrected with the Bonferroni correction (k ⫻ [k ⫺ 1]/2). All statistical analyses were carried out
using SPSS software (version 19; SPSS, Inc, Chicago, Illinois).
aa
Clinical examination
ut
or
iza
This analysis was not the primary purpose of the study, but a
secondary analysis of a total of 78 healthy Danish boys from the
longitudinal part of the COPENHAGEN Puberty Study (11, 12),
which were included with clinical examinations and blood samples drawn every 6 months from 2006 to 2011. Some of these
hormones have reported on previously (13, 14). Participants of
non-Caucasian origin or with no blood sample were excluded
from analyses of the present substudy.
or
Subjects
Co
pi
Pubertal stages were evaluated by clinical examination according to Marshall and Tanner. Testicular volume (TV) was
measured by palpation to the nearest milliliter using the Prader
orchidometer. In the case of a discrepancy between the left and
right side, the largest measurement was used for classification.
Assessment of pubic hair staging was done by visual inspection.
Pubertal onset was defined as TV ⬎ 3 mL in boys.
All evaluations of puberty in the boys were done by 1 of 3 male
pediatricians. Age at onset of pubic hair (PH2⫹) was assigned as
the mean age between ages at first examination in pubic hair
stage 2 and the latest examination in pubic hair stage 1. The same
method was used to determine age at testicular enlargement
(TV ⬎ 3 mL). In 4 of the boys, the age at PH2⫹ was measured
with 6 months accuracy because 12 months elapsed between
examinations. Skinfolds were measured at the biceps, triceps,
subscapular, and iliac crest on the left side of the body using a
Holtain skinfold caliper calibrated to 0.2 mm (Harpenden, British Indicators Ltd, London, United Kingdom).
Hormone analyses
Blood samples were drawn from an antecubital vein between
800 and 1000 hours. They were clotted and centrifuged, and
serum was stored immediately at ⫺20°C until hormone analyses
were performed. Serum LH was measured by time-resolved immunofluorometric assays (Delfia; PerkinElmer, Waltham, Massachusetts) with detection limits of 0.06 and 0.05 IU/L for FSH
and LH, respectively. Intra- and interassay coefficients of vari-
Ethical considerations
The COPENHAGEN Puberty Study was approved by the local
ethics committee (KF 01 282214 and V200.1996/90). The study is
registered in www.ClinicalTrials.gov (identifier NCT01411527).
Results
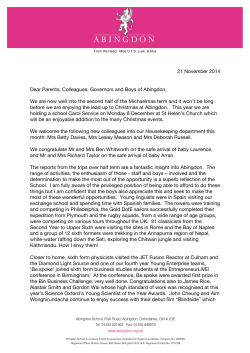
The median AR (CAG)n was 22 (range 17–30) in the 78
healthy boys (Figure 1A). The boys were divided in quartiles (Q1–Q4), according to the length of CAG repeats:
short (Q1), ⱕ20 CAG repeats (25 boys); median (Q2 ⫹
Q3), 21–23 CAG repeats (27 boys); and long (Q4), ⱖ24
CAG repeats (26 boys).
In prepuberty (measured at 10 years of age), the median
sum of skinfolds in boys with long CAG repeats was
25/04/2014
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 24 April 2014. at 14:37 For personal use only. No other uses without permission. . All rights reserved.
J Clin Endocrinol Metab, March 2013, 98(3):E605–E609
14
6
8
25
6
4
a, b
2
17 18 19 20 21 22 23 24 25 26 27 29 30
CAG repeats (number)
3
a
2
b
20
15
10
5
1
0
0
8
9
10
11
12
13
14
C
8
9
10
11
12
13
14
D
300
120
a
200
150
100
a
80
R
Sum of fou
ur skinfolds (mm)
100
60
CD
b
250
SHBG (nmol/l)
30
10
0
4
E607
40
or
LH (IU/l)
5
B
12
Testosterrone (nmol/l)
7
Boys (number)
A
jcem.endojournals.org
20
da
p
50
0
0
9
10
11
12
Age (years)
13
8
14
9
iza
8
10
11
12
13
14
Age (years)
aa
ut
or
Figure 1. Individual assessments of body fat accumulation and serum hormone levels in the group of boys with ⱕ20 CAG repeats (blue lines) 21–
23 CAG repeats (black lines), and ⱖ24 CAG repeats (red lines). Statistical significance representing P ⬍ .05 are given as a (short CAG compared
with medium-length CAG) and b (long CAG compared with medium-length CAG), respectively. A, Levels of LH according to age. B, Levels of
testosterone according to age. C, Levels of SHBG according to age. D, Sum of 4 skinfolds according to age.
Co
pi
41 mm (25th–75 percentile, 31–55 mm) compared with
31 mm in boys with medium-length CAG repeats (23–39
mm) (P ⫽ .06) (Figure 1D), and boys with long CAG
repeats had lower SHBG (88 nmol/L [79 –120 nmol/L])
compared with that of boys with medium-length CAG
repeats (125 nmol/L [94 –156 nmol/L]; P ⫽ .042) (Figure
1C). The inverse association was observed in boys with
short CAG repeats, although not statistically significant at
10 years of age, but at 12 years of age, the boys with short
CAG repeats had statistically significant less body fat compared with both boys with medium-length CAG repeats,
as both BMI and skinfold thickness were lower and SHBG
was higher in puberty (all P ⬍ .05) (Table 1). A positive
linear correlation was observed between CAG length and
skinfold thickness (r ⫽ 0.315 at 10 years and r ⫽ 0.299 at
12 years; both P ⬍ .05) and a negative linear correlation
between CAG length and SHBG (r ⫽ ⫺0.352 at 10 years
and r ⫽ ⫺0.440 at 12 years, P ⬍ .05 and P ⫽ .068,
respectively).
A nonsignificant trend toward younger age at pubarche
(11.4 vs 12.3) years was observed in the group of boys with
long CAG repeats compared with the boys with mediumlength CAG repeats (Table 1).
In puberty, the levels of LH (at 12 years of age) were
significantly higher in boys with short as well as with long
CAG repeats compared with those in boys with mediumlength CAG repeats (all P ⬍ .05). Testosterone (at 12 years
of age) also was higher in boys with long CAG repeats compared with that in boys with medium-length CAG repeats
(P ⬍ .05) (Table 1 and Figure 1, A and B). A large number of
comparisons were conducted, and with a Bonferroni corrected P values statistically significant differences were observed for LH and skinfolds between boys with short CAG
repeats and medium CAG repeats and for LH and testosterone between boys with long CAG repeats and boys with
medium CAG repeats at 12 years of age. No significant association was observed between the length of CAG repeats
and adrenal androgens, DHEAS and ⌬4-androstenedione.
Discussion
In this study of healthy Caucasian boys, we found a median of 22 CAG repeats in the AR gene, which was similar
to the median (21) and distribution found in our previous
study of 116 adult fertile men (6). Likewise, similar dis-
25/04/2014
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 24 April 2014. at 14:37 For personal use only. No other uses without permission. . All rights reserved.
E608
Mouritsen et al
Androgen Receptor CAG Repeats and Body Fat in Boys
J Clin Endocrinol Metab, March 2013, 98(3):E605–E609
Table 1. Clinical and Biochemical Parameters in 78 Healthy Boys at 10, 11, and 12 Years of Age According to AR
CAG Repeat Numbers
Numbers of CAG Repeats
17–20
Median
25thⴚ75th
Percentiles
138.7–148.4
15.8 –17.2
24 –35
107–162
0.01–2.11
0.6 –2.6
0.07– 0.12
⬍0.21–⬍0.21
143.8
17.4
31
125
0.01
1.2
0.1
⬍0.21
137.6 –145.4
16.2–19.1
23–39
94 –156
0.01–1.36
0.6 –1.4
0.04 – 0.09
⬍0.21–⬍0.21
142.6
18.1
41
88a
0.01
1.6
0.1
⬍0.21
137.4 –147.0
16.7–19.8
31–55
79 –120
0.01–1.23
1.2–2.2
0.04 – 0.27
⬍0.21–⬍0.21
145.6
17.6
29
120
1.58
2.2
0.4a
⬍0.21
143.5–152.4
16.8 –18.6
25–36
93–134
0.01–2.58
0.8 –2.7
0.17–1.15
⬍0.21– 0.81
148.1
17.1
35
94
0.01
1.5
0.1
⬍0.21
142.8 –149.8
16.6 –19.6
27– 43
81–132
0.01– 0.81
0.9 –2.3
0.05– 0.56
⬍0.21– 0.11
147.6
18.4
37
85
1.30
1.7
0.4
⬍0.21
141.4 –152.8
17.2–19.5
30 –50
67–111
0.01–2.36
1.2–2.4
0.17– 0.94
⬍0.21– 0.38
149.7
17.1a
28a
115a
1.76
2.6
1.3a
0.98
12.2
11.1
146.8 –156.8
15.6 –17.8
21–33
100 –135
0.01–3.22
1.4 –3.4
1.02–1.89
0.15–1.61
11.4 –12.7
10.8 –11.6
152.2
18.2
49
86
1.47
1.9
0.6
⬍0.21
12.3
11.8
147.4 –155.6
17.4 –21.0
30 – 61
72–112
0.57–1.75
1.4 –2.4
0.45– 0.86
⬍0.21– 0.82
11.2–12.7
10.6 –12.3
155.1
19.4
43
71
2.40
2.4
1.2a
2.2a
11.4
11.5
150.7–160.4
17.7–20.4
29 – 66
52–94
0.80 –3.51
1.8 –3.5
1.01–2.73
0.47– 8.25
10.6 –12.0
10.7–11.9
ut
CD
or
da
p
or
iza
140.2
16.9
29
131
0.61
1.4
0.1
⬍0.21
R
Median
P ⬍ .05 compared with the medium–length group (CAG 21–23).
pi
a
Median
24 –30
25thⴚ75th
Percentiles
aa
At 10 y of age
Height, cm
BMI, kg/m2
Sum of skinfolds, mm
SHBG, nmol/L
Androstenedione, nmol/L
DHEAS, mol/L
LH, IU/L
Testosterone, nmol/L
At 11 y of age
Height, cm
BMI, kg/m2
Sum of skinfolds, mm
SHBG, nmol/L
Androstenedione, nmol/L
DHEAS, mol/L
LH, IU/L
Testosterone, nmol/L
At 12 y of age
Height, cm
BMI, kg/m2
Sum of skinfolds, mm
SHBG, nmol/L
Androstenedione, nmol/L
DHEAS, mol/L
LH, IU/L
Testosterone, nmol/L
Age at PH2⫹, y
Age at TV ⬎3 mL, y
21–23
25thⴚ75th
Percentiles
Co
tributions have been reported in other studies of Caucasian males (7, 15). We observed a nonlinear association
between CAG repeat length and circulating LH and testosterone in early puberty. In contrast, the observed association between CAG repeat length and body fat (and
SHBG) was linear.
We found a greater accumulation of body fat (and
lower serum levels of SHBG) in boys with long CAG repeats (within normal range), but the opposite was found
in boys with short CAG repeats. These findings became
statistically significant after the onset of pubic hair, ie, at
the beginning of puberty, which suggests that androgens
are involved in the physiological mechanisms. This suggestion is consistent with previous findings of higher body
fat content in adult men with longer CAG repeats (16) and
lower BMI or higher muscle mass in men with shorter
CAG repeats (17). Conversely, one study reported a higher
level of fat free mass in adult men with longer CAG, comparing 2 groups divided by the median (⬍22 and ⱖ22)
(18). However, few studies of CAG repeats and body fat
content in boys and adolescents exist. One study of ado-
lescents reported a positive correlation between BMI and
number of CAG repeats (9), whereas another study of boys
from 13 years of age did not confirm such an association
between body composition and CAG repeats (10).
Our longitudinal findings are in line with the Dutch
cross-sectional study of males (13–36 years of age), reporting an earlier pubertal growth spurt in boys with long
CAG repeats but no association between CAG repeat
length and final height (10). Thus, although AR (CAG)n
seem to affect metabolism and reproductive factors in prepubertal boys, the effect of (CAG)n on androgen activity
declines as the serum testosterone concentration increases
after pubertal onset. Earlier fat accumulation in the boys
with long CAG repeat length could be related to the decreased AR signaling in adipocytes, because a study of male
AR knockout mice suggested that AR signaling in adipocytes
protects against high-fat diet–induced obesity (19).
A combination of elevated testosterone, which has been
reported in some studies of adult men with long (CAG)n
(18) and decreased SHBG (20), results in an increased level
of free androgens. The increased level of free androgens
25/04/2014
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 24 April 2014. at 14:37 For personal use only. No other uses without permission. . All rights reserved.
J Clin Endocrinol Metab, March 2013, 98(3):E605–E609
jcem.endojournals.org
could reflect a compensatory mechanism due to decreased
AR sensitivity in boys with long (CAG)n. Furthermore,
long CAG repeat length might be associated with earlier
pubarche.
Limitations of the study are the small sample size and
the performance of multiple comparisons Furthermore,
only Caucasian boys were examined.
In conclusion, our study suggests that longer AR
(CAG)n are associated with increased prepubertal fat accumulation and shorter AR (CAG)n are associated with
less pubertal fat accumulation. Furthermore, nonlinear
associations between CAG length and both LH and testosterone were found in early puberty. Thus, this genetic
variation appears to be important for metabolic and reproductive factors in healthy boys.
5. vis-Dao CA, Tuazon ED, Sokol RZ, Cortessis VK. Male infertility
and variation in CAG repeat length in the androgen receptor gene:
a meta-analysis. J Clin Endocrinol Metab. 2007;92:4319 – 4326.
6. Rajpert-De Meyts E, Leffers H, Petersen JH, et al. CAG repeat length
in androgen-receptor gene and reproductive variables in fertile and
infertile men. Lancet. 2002;359:44 – 46.
7. Nenonen HA, Giwercman A, Hallengren E, Giwercman YL. Nonlinear association between androgen receptor CAG repeat length
and risk of male subfertility—a meta-analysis. Int J Androl. 2011;
34:327–332.
8. Nenonen H, Bjork C, Skjaerpe PA, et al. CAG repeat number is not
inversely associated with androgen receptor activity in vitro. Mol
Hum Reprod. 2010;16:153–157.
9. Lappalainen S, Utriainen P, Kuulasmaa T, Voutilainen R, Jaaskelainen J. Androgen receptor gene CAG repeat polymorphism and
X-chromosome inactivation in children with premature adrenarche.
J Clin Endocrinol Metab. 2008;93:1304 –1309.
10. Voorhoeve PG, van Mechelen W, Uitterlinden AG, Delemarre-van
de Waal HA, Lamberts SW. Androgen receptor gene CAG repeat
polymorphism in longitudinal height and body composition in children and adolescents. Clin Endocrinol (Oxf). 2011;74:732–735.
11. Aksglaede L, Sorensen K, Petersen JH, Skakkebaek NE, Juul A.
Recent decline in age at breast development: the Copenhagen Puberty Study. Pediatrics. 2009;123:e932– e939.
12. Sorensen K, Aksglaede L, Petersen JH, Juul A. Recent changes in
pubertal timing in healthy Danish boys: associations with body mass
index. J Clin Endocrinol Metab. 2010;95:263–270.
13. Mouritsen A, Aksglaede L, Sorensen K, et al. The pubertal transition
in 179 healthy Danish children: associations between pubarche, adrenarche, gonadarche and body composition. Eur J Endocrinol
2012;168:129 –136.
14. Aksglaede L, Sorensen K, Boas M, et al. Changes in anti-Mu¨llerian
hormone (AMH) throughout the life span: a population-based study
of 1027 healthy males from birth (cord blood) to the age of 69 years.
J Clin Endocrinol Metab. 2010;95:5357–5364.
15. Travison TG, Shackelton R, Araujo AB, et al. Frailty, serum androgens, and the CAG repeat polymorphism: results from the Massachusetts Male Aging Study. J Clin Endocrinol Metab. 2010;95:
2746 –2754.
16. Zitzmann M, Gromoll J, von Eckardstein A, Nieschlag E. The CAG
repeat polymorphism in the androgen receptor gene modulates body
fat mass and serum concentrations of leptin and insulin in men.
Diabetologia. 2003;46:31–39.
17. Nielsen TL, Hagen C, Wraae K, et al. The impact of the CAG repeat
polymorphism of the androgen receptor gene on muscle and adipose
tissues in 20⫺29-year-old Danish men: Odense Androgen Study.
Eur J Endocrinol. 2010;162:795– 804.
18. Walsh S, Zmuda JM, Cauley JA, et al. Androgen receptor CAG
repeat polymorphism is associated with fat-free mass in men. J Appl
Physiol. 2005;98:132–137.
19. McInnes KJ, Smith LB, Hunger NI, Saunders PT, Andrew R, Walker
BR. Deletion of the androgen receptor in adipose tissue in male mice
elevates retinol binding protein 4 and reveals independent effects on
visceral fat mass and on glucose homeostasis. Diabetes. 2012;61:
1072–1081.
20. Sorensen K, Aksglaede L, Munch-Andersen T, et al. Sex hormonebinding globulin levels predict insulin sensitivity, disposition index
and cardiovascular risk during puberty. Diabetes Care. 2009;32:
909 –914.
or
da
p
Address all correspondence and requests for reprints
to: Annette Mouritsen, University Department of Growth
and Reproduction, Rigshospitalet, Section 5064. E-mail:
[email protected].
CD
R
Acknowledgments
Co
pi
aa
ut
or
iza
This study was supported by the Sawmill Owner Jeppe Juhl
and wife Ovita Juhls Memorial Fund, Aase and Einar Danielsen
Foundation, Kirsten and Freddy Johansen Foundation, European Union FP7 (DEER; Grant Agreement 212844), and Danish
Agency for Science, Technology and Innovation 09-067180
Danish Council for Strategic Research 2009 (DAN-ED; Grant
Agreement 2107-05-0006).
The study is registered in www.ClinicalTrials.gov Identifier:
NCT01411527.
Disclosure Summary: The authors have nothing to disclose.
References
1. Lubahn DB, Joseph DR, Sullivan PM, Willard HF, French FS, Wilson EM. Cloning of human androgen receptor complementary DNA
and localization to the X chromosome. Science. 1988;240:327–330.
2. La Spada AR, Wilson EM, Lubahn DB, Harding AE, Fischbeck KH.
Androgen receptor gene mutations in X-linked spinal and bulbar
muscular atrophy. Nature. 1991;352:77–79.
3. Chamberlain NL, Driver ED, Miesfeld RL. The length and location
of CAG trinucleotide repeats in the androgen receptor N-terminal
domain affect transactivation function. Nucleic Acids Res. 1994;
22:3181–3186.
4. Tut TG, Ghadessy FJ, Trifiro MA, Pinsky L, Yong EL. Long polyglutamine tracts in the androgen receptor are associated with reduced trans-activation, impaired sperm production, and male infertility. J Clin Endocrinol Metab. 1997;82:3777–3782.
E609
25/04/2014
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 24 April 2014. at 14:37 For personal use only. No other uses without permission. . All rights reserved.
© Copyright 2026 ExpyDoc