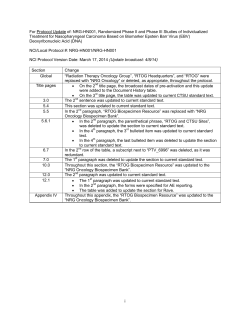
Published Ahead of Print on April 15, 2013 as 10.1200/JCO.2012.45.3282 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2012.45.3282 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Randomized Phase II Study of Ixabepilone or Paclitaxel Plus Carboplatin in Patients With Non–Small-Cell Lung Cancer Prospectively Stratified by Beta-3 Tubulin Status Martin J. Edelman, Claus-Peter Schneider, Chun-Ming Tsai, Heung-Tae Kim, Elisabeth Quoix, Alexander V. Luft, Remigiusz Kaleta, Pralay Mukhopadhyay, Ovidiu C. Trifan, Laura Whitaker, and Martin Reck Martin J. Edelman, University of Maryland Greenebaum Cancer Center, Baltimore, MD; Claus-Peter Schneider, Zentralklinik Bad Berka, Bad Berka; Martin Reck, Hospital Grosshansdorf, Grosshansdorf, Germany; Chun-Ming Tsai, Taipei Veterans General Hospital, Taipei, Taiwan; Heung-Tae Kim, National Cancer Center, Goyang-Si, Korea; Elisabeth Quoix, Nouvel Hopital Civil, Strasbourg, France; Alexander V. Luft, Leningrad Regional Clinical Hospital, St Petersburg, Russia; and Remigiusz Kaleta, Pralay Mukhopadhyay, Ovidiu C. Trifan, and Laura Whitaker, Bristol-Myers Squibb, Wallingford, CT. Published online ahead of print at www.jco.org on April 15, 2013. Supported by Bristol-Myers Squibb. Authors’ disclosures of potential conflicts of interest and author contributions are found at the end of this article. Clinical trial information: NCT00723957. Corresponding author: Martin J. Edelman, MD, University of Maryland Greenebaum Cancer Center, Division of Hematology/Oncology, 22 South Green St, Baltimore, MD 21201-1595; e-mail: [email protected]. © 2013 by American Society of Clinical Oncology 0732-183X/13/3199-1/$20.00 A B S T R A C T Purpose Retrospective studies have reported that tumor expression of the beta-3 tubulin (3T) isoform is an unfavorable prognostic factor in non–small-cell lung cancer (NSCLC) treated with tubulininhibiting chemotherapy. Ixabepilone is a tubulin-inhibiting agent with low susceptibility to multiple resistance mechanisms including 3T isoform expression in several tumor models. This randomized phase II study evaluated ixabepilone-based chemotherapy in stage IIIb/IV NSCLC, compared with paclitaxel-based chemotherapy. Tumor specimens were prospectively evaluated for 3T expression. Patients and Methods Patients were stratified by 3T status (positive v negative) and randomly assigned at a ratio of 1:1 to receive ixabepilone (32 mg/m2) and carboplatin (area under concentration-time curve [AUC], 6) or paclitaxel (200 mg/m2) and carboplatin (AUC, 6) for up to six cycles. The primary end point was progression-free survival (PFS) in the 3T-positive subgroup. Results Ninety-five patients (3T positive, 52; 3T negative, 43) received ixabepilone plus carboplatin; 96 patients (3T positive, 49; 3T negative, 47) received paclitaxel plus carboplatin. No significant differences in median PFS were observed between arms for either subgroup (3T positive, 4.3 months in both arms; 3T negative, 5.8 v 5.3 months). Ixabepilone did not significantly improve overall survival (OS) for the 3T-positive subset or the overall population. Adverse events were similar between the two arms and comparable with those in previous studies. Conclusion There was no predictive value of 3T in differentiating clinical activity of ixabepilone- or paclitaxel-containing regimens. Ixabepilone did not improve PFS or OS in patients with 3Tpositive tumors. 3T-positive patients had worse PFS relative to 3T-negative patients, regardless of treatment; hence, 3T expression seems to be a negative prognostic factor, but not a predictive factor, in advanced NSCLC treated with either ixabepilone or paclitaxel platinum-based doublets. J Clin Oncol 31. © 2013 by American Society of Clinical Oncology DOI: 10.1200/JCO.2012.45.3282 INTRODUCTION Currently accepted first-line chemotherapy for stage IV non–small-cell lung cancer (NSCLC) includes a platinum-based agent in combination with vinorelbine, gemcitabine, or a taxane.1,2 The combinations of platinum plus pemetrexed and platinum, paclitaxel, and bevacizumab have recently demonstrated some advantage over other regimens in nonsquamous carcinoma.3,4 In an attempt to individualize treatment to improve patient survival and effectiveness of therapy, clinical research has been focused on identification of biologic markers that are either prognostic and/or predictive of response to specific cytotoxic drugs (eg, DNA repair enzymes, ribonucleotide subunits, and beta-3 tubulin [3T]).5,6 Increased 3T expression is associated with an increased rate of metastasis, and it is thought that expression levels of 3T might be predictive for response to chemotherapy, especially taxanes.7 Several studies have indicated that 3T overexpression might be a common mechanism for taxane resistance in advanced tumors.8-10 Epothilones are a novel class of antimicrotubule agents, which, similarly to taxanes, bind to and stabilize microtubules, thereby resulting in mitotic © 2013 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved. Copyright 2013 by American Society of Clinical Oncology 1 Edelman et al arrest at G2/M transition.11 Ixabepilone, a semisynthetic, metabolically stable derivative of epothilone B, has shown clinical activity in several tumor types, especially in tumors resistant to other cytotoxic agents.12,13 Of interest, several preclinical studies have demonstrated activity of ixabepilone in taxane-resistant disease. The taxane-resistant breast cancer model Pat-21 demonstrates overexpression of 3T but is sensitive to an epothilone.14 Additional studies have demonstrated activity with ixabepilone in the 3T-overexpressing NSCLC tumor models H1155 and LX-1, which are refractory to docetaxel and vinorelbine.15 In a phase II study of patients with advanced NSCLC previously treated with a platinum-containing regimen, single-agent ixabepilone demonstrated clinically relevant activity.16 Significantly, responses were seen in patients who had progressed after taxanecontaining therapy. Given the antitumor activity of ixabepilone in taxane-resistant tumors and the observation that tumors overexpressing 3T respond poorly to taxanes, we hypothesized that ixabepilone may show clinical activity superior to that of paclitaxel when administered as initial combination treatment with carboplatin to patients with NSCLC who have tumors that overexpress 3T. Here, we present the results of a phase II study of ixabepilone plus carboplatin versus paclitaxel plus carboplatin in patients with advanced NSCLC who were prospectively analyzed and stratified based on 3T status. PATIENTS AND METHODS Study Design and Treatment This was a randomized, international, multicenter, open-label, phase II study of ixabepilone in combination with carboplatin, compared with paclitaxel and carboplatin, in patients with NSCLC who had not received any systemic therapy for their cancer. Patients were randomly assigned at a ratio of 1:1 and stratified by tumor expression level of 3T (positive v negative), disease stage (stage IIIb v IV), presence of brain metastases (yes v no), and study site to one of the following arms: ixabepilone administered as a 3-hour intravenous infusion at a starting dose of 32 mg/m2 on day 1 of a 21-day cycle, consistent with a previous phase II trial of single-agent ixabepilone,16 followed by carbo- platin administered at a dose calculated to produce an area under the concentration-time curve of 6 mg/mL/min on day 1 of a 21-day cycle; or paclitaxel administered as a 3-hour intravenous infusion at a starting dose of 200 mg/m2 on day 1 of a 21-day cycle followed by carboplatin (area under concentration-time curve, 6) administered on day 1 of a 21-day cycle. The recommended phase II dose of ixabepilone and carboplatin was determined as 30 mg/m2 in a previously reported phase I study17; however, a dose of 32 mg/m2 was used in this study, consistent with that used as a second-line single agent in a previous phase II study.16 All randomly assigned patients were to be treated for a maximum of six cycles or until disease progression or unacceptable toxicity. The protocol was conducted in accordance with Good Clinical Practice, as defined by the International Conference on Harmonisation and in accordance with the ethical principles underlying European Union Directive 2001/ 20/EC and US Code of Federal Regulations, Title 21, Part 50. Before initiation, this study was approved by the institutional review board or independent ethics committee at each site. All patients provided written informed consent. Patients Eligible patients were men and women age ⱖ 18 years who had histologically confirmed NSCLC (stage IIIb with pleural effusion, stage IV disease, or recurrent disease after surgery and/or radiation therapy), Karnofsky performance status of 70 to 100, and life expectancy of at least 3 months. Availability of paraffin-embedded tissue (to measure expression levels of 3T) and measurable disease by RECIST (version 1.0) guidelines with at least one target lesion outside of a previous radiotherapy field were required for study entry. Patients with known uncontrolled brain metastases were excluded from the study, and those with known metastases were required to have a baseline imaging scan within 4 weeks of random assignment; patients with peripheral neuropathy grade ⬎ 1 were also excluded. Radiation therapy or major surgery and focal/palliative radiation therapy or minor surgery were to be completed 4 weeks and 1 week before random assignment, respectively. Patients with inadequate hematologic (absolute neutrophil count [ANC] ⬍ 1,500 cells/L, hemoglobin ⬍ 9.0 g/dL, and platelets ⬍ 100,000 cells/L), hepatic (total bilirubin ⬎ upper limit of normal), or renal function (serum creatinine ⱖ 1.5 mg/dL; calculated creatinine clearance based on Cockcroft-Gault ⬍ 50 mL/ min) were excluded. Study Assessments 3T expression levels in tissue specimens were assessed using immunohistochemistry (IHC) staining. Tissue sections that either had available Random assignment (N = 197) Ixabepilone + carboplatin Received treatment Did not receive treatment (n = 98) (n = 95) (n = 3) Paclitaxel + carboplatin Received treatment Did not receive treatment ((n n=9 99) 8) (n = 96) (n = 3) Fig 1. CONSORT diagram; patient disposition. AE, adverse event. Completed treatment Still on treatment Discontinued treatment Disease progression Study drug toxicity AE unrelated to study drug Death Patient request Maximum clinical benefit Withdrawal of consent Other 2 (n = 47) (n = 1) (n = 27) (n = 4) (n = 1) (n = 3) (n = 3) (n = 4) (n = 4) (n = 1) © 2013 by American Society of Clinical Oncology Completed treatment Still on treatment Discontinued treatment Disease progression Study drug toxicity AE unrelated to study drug Death Patient request Maximum clinical benefit Withdrawal of consent Other (n = 46) (n = 0) (n = 25) (n = 6) (n = 4) (n = 4) (n = 3) (n = 5) (n = 2) (n = 1) JOURNAL OF CLINICAL ONCOLOGY Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved. Ixabepilone Plus Carboplatin in Advanced NSCLC Table 1. Baseline Patient Demographics and Clinical Characteristics Ixabepilone Plus Carboplatin (n ⫽ 98) Characteristic (overall population) Age, years Median Range Sex Male Female Ethnicity White Asian Other Tumor histology Adenocarcinoma Bronchioloalveolar carcinoma Large-cell carcinoma Squamous cell carcinoma Other/unknown Karnofsky performance status, % 100 90 80 70 Not reported 3Tⴱ Positive Negative Disease stageⴱ IIIb IV Presence of brain metastasisⴱ No Yes Smoking status Current Former Never Unknown No. % 60.0 29.0-80.0 % 60.0 34.0-85.0 73.5 26.5 67 32 67.7 32.3 68 30 0 69.0 30.6 0.0 76 22 1 76.8 22.2 1.0 51 1 3 38 5 52.0 1.0 3.1 38.8 5.1 55 0 5 34 5 55.6 0.0 5.1 34.3 5.1 9 35 41 13 0 9.2 35.7 41.8 13.3 0.0 10 43 35 10 1 10.1 43.4 35.4 10.1 1.0 53 45 54.1 45.9 51 48 51.5 48.5 7 91 7.1 92.9 8 91 8.1 91.9 89 9 90.8 9.2 90 9 90.9 9.1 49 28 18 3 50.0 28.6 18.4 3.1 43 31 22 3 43.4 31.3 22.2 3.0 No. % Age, years Median 60.0 Range 29.0-80.0 Sex Male 40 75.5 Female 13 24.5 Karnofsky performance status, % 100 5 9.4 90 15 28.3 80 24 45.3 70 9 17.0 Not reported 0 0.0 Tumor histology Adenocarcinoma 30 56.6 Bronchioloalveolar carcinoma 1 1.9 (continued in next column) www.jco.org No. 72 26 Ixabepilone Plus Carboplatin (n ⫽ 53) Characteristic (3T-positive patients) Paclitaxel Plus Carboplatin (n ⫽ 99) Paclitaxel Plus Carboplatin (n ⫽ 51) No. % 60.0 43.0-80.0 32 19 62.7 37.3 7 22 16 5 1 13.7 43.1 31.4 9.8 2.0 33 0 64.7 0.0 Table 1. Baseline Patient Demographics and Clinical Characteristics (continued) Ixabepilone Plus Carboplatin (n ⫽ 53) Characteristic (3T-positive patients) Large-cell carcinoma Squamous cell carcinoma Other/unknown Paclitaxel Plus Carboplatin (n ⫽ 51) No. % No. % 2 17 3 3.8 32.1 5.7 2 13 3 3.9 25.5 5.9 Abbreviation: 3T, beta-3 tubulin. ⴱ Stratification factor. formalin-fixed, paraffin-embedded tumor tissue or required rebiopsy of tumor tissue were submitted to Dako North America (Carpinteria, CA) for 3T IHC analysis. Formalin-fixed, paraffin-embedded tissue blocks were sectioned and adhered to positively charged glass slides. 3T staining was assessed using a prototype pharmacodiagnostic IHC assay that was optimized by Dako (Glostrup, Denmark). The assay was based on previously reported IHC assays for 3T.8,18 Tissue sections that contained ⱖ 50% of tumor cells staining at ⱖ 2⫹ intensity (on scale of 0, 1⫹, 2⫹, and 3⫹, where 0 was no staining and 3⫹ was maximum intensity) were scored as 3T positive, whereas all others were scored as 3T negative. Endothelial cells within tissue sections consistently stained at an intensity ⱖ 2⫹ with this assay and thus served as an internal positive control. 3T testing was performed before random assignment, and 3T status was used as a stratification factor at random assignment. Tumor evaluations (physical examination and imaging studies) were performed at baseline and every 6 weeks during treatment until documented disease progression. Response was assessed according to revised RECIST (version 1.0), with a repeat assessment to confirm response performed at ⱖ 4 weeks. Patients with objective responses who discontinued treatment for reasons other than disease progression were to undergo regular tumor assessment until disease progression. All patients underwent physical examination, including vital signs and performance status, serum chemistries (lactate dehydrogenase, blood urea nitrogen or urea, creatinine, ALT, AST, alkaline phosphatase, and total bilirubin), and hematology (complete blood count plus differential and platelets) before random assignment. Thereafter, hematology was evaluated weekly, and serum chemistry was evaluated before each cycle. Creatinine clearance based on Cockroft-Gault was calculated before each cycle. Toxicities were evaluated continuously during the treatment phase, and patients who experienced any drug-related toxicity were observed at least every 4 weeks during the follow-up phase until the toxicities were resolved, were stabilized, returned to baseline, or were deemed irreversible. Adverse events, laboratory values, and other symptoms were graded according to the National Cancer Institute Common Toxicity Criteria (version 3.0). Toxicities requiring a dose reduction were ANC ⬍ 500/L lasting ⱖ 5 days, febrile neutropenia, platelets ⬍ 25,000/L, grade 4 hemoglobin, grade 3 nausea/vomiting, grade 3 stomatitis, grade 3 diarrhea, neuropathy (grade 2 lasting ⬎ 7 days or grade 3 lasting ⬍ 7 days), and other grade ⱖ 3 toxicities. Patients experiencing grade 3 neuropathy lasting ⱖ 7 days or grade 4 neuropathy were to discontinue treatment with ixabepilone and paclitaxel. Retreatment criteria included ANC ⬎ 1500/L, platelets ⬎ 100,000/L, and resolution of treatment-related nonhematologic toxicity to baseline or grade ⱕ 1 (excluding grade 2 alopecia and grade 2 fatigue). Patients with grade 2 neuropathy were not re-treated until improvement to grade 1 or 0. Patients who did not recover from a treatment-related toxicity to baseline or grade ⱕ 1 within 3 weeks of scheduled re-treatment were required to discontinue using the drug causing the delay or discontinue study participation. Patients requiring more than two dose reductions from any of the study drugs were also required to discontinue study participation. No dose re-escalations were permitted during the study. © 2013 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved. 3 Edelman et al A Ixa + carb Pac + carb Progression-Free Survival (proportion) 1.0 0.8 Stratified log-rank P = .632 0.6 0.4 0.2 0 2 98 99 Efficacy The primary end point of the study was a comparison of PFS between patients with 3T-positive tumors receiving carboplatin plus paclitaxel versus carboplatin plus ixabepilone (Fig 2). For the subgroup of patients with 3T-positive tumors, median PFS was 4.3 months in both treatment arms (Fig 2C; ixabepilone plus carboplatin: 80% CI, 3.2 to 4.9; paclitaxel plus carboplatin: 80% CI, 4.0 to 5.4; HR, 1.04; 80% CI, 0.78 to 1.41; P ⫽ .853). Therefore, the primary end point of the study was not met. In the overall patient population, median 4 © 2013 by American Society of Clinical Oncology 10 12 14 16 22 26 69/98 75/99 15 11 4 4 2 1 0 1 0 0 Median (80% CI) HR (80% CI) 5.3 (4.3 to 5.7) 5.1 (4.3 to 5.6) 0.92 (0.73 to 1.15) Ixa + carb Pac + carb Stratified log-rank P = .35 0.6 0.4 0.2 2 4 6 8 10 12 14 16 1 0 0 0 0 0 Time (months) 45 48 36 36 24 28 11 11 No. Progressed/ No. Randomly Assigned Ixa + carb Pac + carb Ixa + carb over pac + carb 27/45 35/48 9 4 3 3 Median (80% CI) HR (80% CI) 5.8 (5.3 to 6.8) 5.3 (4.4 to 5.8) 0.78 (0.55 to 1.10) Ixa + carb Pac + carb 1.0 0.8 Stratified log-rank P = .853 0.6 0.4 0.2 0 No. at risk Ixa + carb Pac + carb Group 52 57 0.8 No. at risk Ixa + carb Pac + carb C 8 1.0 0 Progression-Free Survival (proportion) Patients and Treatment A total of 197 patients with treatment-naive NSCLC were randomly assigned to receive either ixabepilone plus carboplatin (n ⫽ 98) or paclitaxel plus carboplatin (n ⫽ 99) at 33 sites across 10 countries from December 2, 2008, to February 23, 2010. Of these, 191 patients were treated as follows: 95 with ixabepilone plus carboplatin and 96 with paclitaxel plus carboplatin (Fig 1). The baseline demographics and disease characteristics were well balanced between the groups, including the subgroup of patients with 3T-positive tumors (Table 1). Patients in the ixabepilone plus carboplatin arm received a median of six cycles (range, one to six) of ixabepilone as well as carboplatin. Patients in the paclitaxel plus carboplatin received a median of five cycles (range, one to six) of paclitaxel and carboplatin. 76 75 Ixa + carb Pac + carb Ixa + carb over pac + carb Group RESULTS 6 No. Progressed/ No. Randomly Assigned Group B 4 Time (months) No. at risk Ixa + carb Pac + carb Progression-Free Survival (proportion) Statistical Analysis The primary objective of this study was to test the hypothesis that progression-free survival (PFS) in the ixabepilone plus carboplatin arm would be superior to PFS in the paclitaxel plus carboplatin arm for the 3T-positive subgroup. The sample size was calculated to provide 90% power to detect a statistically significant difference in PFS between the two arms for the 3Tpositive subgroup using a two-sided ␣ ⫽ 0.2 log-rank test, if the true hazard ratio (HR) were 0.58 (assuming median PFS of 3.2 v 5.5 months). Secondary study objectives included comparing PFS for the entire population between the two arms, estimating tumor response rates and survival in both arms, and evaluating safety of the ixabepilone plus carboplatin combination. Patients with 3T-negative tumors were also enrolled onto the study to estimate the treatment effect in this subgroup and evaluate the predictive and prognostic value of the biomarker. PFS (time from random assignment to date of progression or death) was estimated using Kaplan-Meier methodology. For the 3T-positive subgroup, comparison of PFS between treatment arms was carried out using a two-sided ␣ ⫽ 0.2 log-rank test stratified by disease stage (stage IIIb v IV) and presence of brain metastases (yes v no). An unadjusted Cox proportional hazards model stratified by disease stage (stage IIIb v IV) and presence of brain metastases (yes v no) was used to compute PFS HR and the associated two-sided 80% CI. In addition, one-sided P values for log-rank tests and one-sided 90% CIs for HRs were also reported. Two-sided 80% CIs for median PFS were calculated for each treatment arm. The 95% CIs for the medians were also reported. Similar methods were used for comparing PFS between the two arms for the entire population; however, the log-rank test and unadjusted Cox proportional hazards model were stratified by 3T expression level (positive v negative), disease stage (stage IIIb v IV), and presence of brain metastases (yes v no). For the 3T-negative subgroup, median PFS for each treatment arm and HRs along with 80% CIs were reported. Response and disease control rates and respective 80% CIs were estimated for each arm for the 3T-positive subgroup, 3T-negative subgroup, and overall population. Similar analyses, as for PFS, were also conducted for overall survival (OS) in the 3T-positive and -negative subsets and the overall population. 2 4 6 8 10 12 14 16 1 1 0 1 0 0 Time (months) 53 51 40 39 28 29 11 15 No. Progressed/ No. Randomly Assigned Ixa + carb Pac + carb Ixa + carb over pac + carb 42/53 40/51 6 7 1 1 Median (80% CI) HR (80% CI) 4.3 (3.2 to 4.9) 4.3 (4.0 to 5.4) 1.04 (0.78 to 1.41) Fig 2. Progression-free survival in (A) overall patient population, (B) beta-3 tubulin (3T) –negative patients, and (C) 3T-positive patients. Carb, carboplatin; HR, hazard ratio; Ixa, ixabepilone; Pac, paclitaxel. PFS was 5.3 months (80% CI, 4.3 to 5.7) for ixabepilone plus carboplatin and 5.1 months (80% CI, 4.3 to 5.6) for patients treated with paclitaxel plus carboplatin (Fig 2A; HR, 0.92; 80% CI, 0.73 to 1.15; P ⫽ .632). For the 3T-negative subgroup of patients, median PFS was JOURNAL OF CLINICAL ONCOLOGY Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved. Ixabepilone Plus Carboplatin in Advanced NSCLC Overall Survival (proportion) 1.0 Ixa + carb Pac + carb Censored Censored 0.8 0.6 0.4 0.2 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 Time (months) No. at risk Positive 104 94 87 77 61 51 44 36 27 22 21 15 10 Negative 93 83 74 64 54 45 41 34 30 28 18 11 9 Group No. of Deaths/ No. Randomly Assigned Positive Negative Positive over negative 80/104 57/93 Median (80% CI) 7 1 4 0 2 0 0 0 HR (80% CI) 10.6 (9.2 to 12.4) 13.1 (10.7 to 14.5) 1.16 (0.92 to 1.46) Fig 3. Overall survival by beta-3 tubulin status (positive v negative). Carb, carboplatin; HR, hazard ratio; Ixa, Ixabepilone; Pac, paclitaxel. 5.8 months (80% CI, 5.3 to 6.8) for ixabepilone plus carboplatin and 5.3 months (80% CI, 4.4 to 5.8) for paclitaxel plus carboplatin (Fig 2B; HR, 0.78; 80% CI, 0.55 to 1.10; P ⫽ .350). OS, a secondary end point of the trial, also did not favor the ixabepilone arm in the 3T-positive subset. In this subgroup, the median OS for ixabepilone plus carboplatin was 10.61 months (80% CI, 7.79 to 12.42); it was 11.37 months (80% CI, 9.23 to 13.93) for patients treated with paclitaxel plus carboplatin (HR, 1.60; 80% CI, 1.20 to 2.10; P ⫽ .053). For the 3T-negative subgroup, the median OS for ixabepilone plus carboplatin was 16.92 months (80% CI, 14.26 to 23.56); it was 9.40 months (80% CI, 8.25 to 12.29) for patients treated with paclitaxel plus carboplatin (HR, 0.70; 80% CI, 0.50 to 0.90; P ⫽ .123). In the overall population, the median OS was 13.04 months (80% CI, 10.74 to 14.26) for ixabepilone plus carboplatin; it was 10.15 months (80% CI, 9.00 to 12.29) for paclitaxel plus carboplatin (HR, 1.10; 80% CI, 0.90 to 1.40; P ⫽ .622). Because of the observed differences in OS, noted in the 3Tnegative subgroup, additional exploratory analyses were conducted to understand these results. In particular, a multivariate Cox regression analysis was conducted, adjusting for the following prognostic factors: sex, age, performance status, ethnicity, and smoking status. When adjusted using the Cox regression model, the HR was 0.777 (80% CI, 0.528 to 1.144; P ⫽ .4030) in the 3T-negative subset. In the 3Tpositive subset, the HR was 1.497 (80% CI, 1.083 to 2.070; P ⫽ .1106) using the multivariate analysis; in the overall population, the HR was 1.035 (80% CI, 0.817 to 1.311; P ⫽ .8526). 3T positivity has been described as a negative prognostic factor. We evaluated PFS and OS in patients who were 3T positive (n ⫽ 104) versus patients who were 3T negative (n ⫽ 93). PFS for 3T-positive patients was 4.27 months (80% CI, 3.61 to 5.42); it was 5.59 months (80% CI, 4.63 to 6.47) for 3T-negative patients (HR, 1.32; 80% CI, 1.06 to 1.64). The OS for 3T-positive patients was 10.6 months (80% CI, 9.2 to 12.4); it was 13.1 months (80% CI, 10.7 to 14.5) for 3T-negative patients (HR, 1.16; 80% CI, 0.92 to 1.46; Fig 3). The response rate for the ixabepilone plus carboplatin arm was numerically lower than that for the paclitaxel plus carboplatin arm in the subpopulation of patients with 3T-positive tumors (17%; 95% CI, 8 to 30 v 29%; 95% CI, 18 to 44; Table 2). Similar results were seen in the overall population, with response rates of 21% (95% CI, 14 to 31) and 28% (95% CI, 20 to 38) in the corresponding arms. An identical response rate of 27% (95% CI, 15 to 42) was noted for the two treatment arms in the subpopulation of patients with 3T-negative tumors. An overall disease control rate of 77% to 78% was observed in both treatment arms in the 3T-positive and -negative subpopulations as well as in the overall patient population (Table 2). A summary of efficacy results is presented in Appendix Tables A1 and A2 (online only). Safety Adverse events were similar between the two arms and comparable to those seen in previous studies (Table 3). Treatment-related adverse events were mostly mild to moderate (grade 1 or 2) in severity. No grade 4 nonhematologic adverse events were reported. Table 2. Response Rates 3T Positive Ixabepilone Plus Carboplatin (n ⫽ 53) 3T Negative Paclitaxel Plus Carboplatin (n ⫽ 51) Ixabepilone Plus Carboplatin (n ⫽ 45) Overall Population Paclitaxel Plus Carboplatin (n ⫽ 48) Ixabepilone Plus Carboplatin (n ⫽ 98) Paclitaxel Plus Carboplatin (n ⫽ 99) Response No. % No. % No. % No. % No. % No. % Tumor response CR PR SD PD NDⴱ Response rate† Disease control rate‡ 1 8 32 10 2 9 41 1.9 15.1 60.4 18.9 3.8 17.0 77.4 2 13 24 7 5 15 39 3.9 25.5 47.1 13.7 9.8 29.4 76.5 0 12 23 4 6 12 35 0.0 26.7 51.1 8.9 13.3 26.7 77.8 0 13 24 7 4 13 37 0.0 27.1 50.0 14.6 8.3 27.1 77.1 1 20 55 14 8 21 76 1.0 20.4 56.1 14.3 8.2 21.4 77.6 2 26 48 14 9 28 76 2.0 26.3 48.5 14.1 9.1 28.3 76.8 Abbreviations: 3T, beta-3 tubulin; CR, complete response; ND, not determined; PD, progressive disease; PR, partial response; SD, stable disease. ⴱ Data unavailable because of early discontinuation or death or because patient was never treated in study. †CR ⫹ PR/No. of patients. ‡CR ⫹ PR ⫹ SD/No. of patients. www.jco.org © 2013 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved. 5 Edelman et al Table 3. Toxicity Ixabepilone Plus Carboplatin (n ⫽ 95) Any Grade Grade 3 Paclitaxel Plus Carboplatin (n ⫽ 96) Grade 4 Any Grade Grade 3 Grade 4 Hematologic AE No. % No. % No. % No. % No. % No. % Neutropenia Anemia Thrombocytopenia Leukopenia 74 89 64 74 82.2 98.9 71.1 82.2 19 11 10 28 21.1 12.2 11.1 31.1 35 4 4 3 38.9 4.4 4.4 3.3 73 84 49 65 79.3 90.3 52.7 69.9 29 0 1 15 31.5 0.0 1.1 16.1 22 0 0 0 23.9 0.0 0.0 0.0 Ixabepilone Plus Carboplatin (n ⫽ 95) Any Grade Nonhematologic AE ⴱ Neurologic Peripheral sensory neuropathy† Skin Alopecia Pruritus GI Nausea Vomiting Diarrhea Upper abdominal pain Constipation General/administration site Fatigue Asthenia Pain Pyrexia Metabolic Decreased appetite Musculoskeletal/connective tissue Arthralgia Myalgia Grade 3 Paclitaxel Plus Carboplatin (n ⫽ 96) Grade 4 Any Grade Grade 3 Grade 4 No. % No. % No. % No. % No. % No. % 35 36.8 0 0.0 0 0.0 54 56.3 7 7.3 0 0.0 45 3 47.4 3.2 NA 0 0.0 NA 0 0.0 55 6 57.3 6.3 NA 1 1.0 NA 0 0.0 39 16 13 5 5 41.1 16.8 13.7 5.3 5.3 1 1 2 0 0 1.1 1.1 2.1 0.0 0.0 0 0 0 0 0 0.0 0.0 0.0 0.0 0.0 29 8 9 1 6 30.2 8.3 9.4 1.0 6.3 1 1 1 0 0 1.0 1.0 1.0 0.0 0.0 0 0 0 0 0 0.0 0.0 0.0 0.0 0.0 29 11 6 6 30.5 11.6 6.3 6.3 1 1 0 0 1.1 1.1 0.0 0.0 0 0 0 0 0.0 0.0 0.0 0.0 24 14 4 2 25.0 14.6 4.2 2.1 2 2 0 0 2.1 2.1 0.0 0.0 0 0 0 0 0.0 0.0 0.0 0.0 29 30.5 1 1.1 0 0.0 24 25.0 1 1.0 0 0.0 15 15 15.8 15.8 0 0 0.0 0.0 0 0 0.0 0.0 22 27 22.9 28.1 2 2 2.1 2.1 0 0 0.0 0.0 Abbreviations: AE, adverse event; NA, not applicable. ⴱ Treatment-related AEs in ⱖ 5% of patients in either treatment arm. †Includes the following Medical Dictionary for Regulatory Activities (version 9.1) terms: neuralgia, neuropathy peripheral, paraesthesia, peripheral sensory neuropathy, neurotoxicity, and polyneuropathy. Within 30 days of receiving the study drug, there were three deaths in the ixabepilone plus carboplatin arm and five deaths in the paclitaxel plus carboplatin arm. The three deaths in the ixabepilone plus carboplatin arm resulted from cardiac events (one ventricular fibrillation, one heart failure, and one sudden cardiac arrest). Given the high incidence of coexisting cardiac disease in the lung cancer population, these events were most likely not related to the drug. In the ixabepilone plus carboplatin group, 30% and 38% of patients had at least one dose reduction of ixabepilone and/or carboplatin, respectively. In the paclitaxel plus carboplatin arm, at least 23% and 25% of patients had at least one dose reduction of paclitaxel and/or carboplatin, respectively. DISCUSSION Cytotoxic chemotherapy has unequivocally been associated with benefit in NSCLC. In advanced disease, chemotherapy improves both quality and quantity of life, albeit modestly. Despite these benefits, it is clear that a substantial number of patients do not obtain benefit and experience toxicity as a consequence of treatment. Although new 6 © 2013 by American Society of Clinical Oncology so-called targeted agents have also demonstrated benefit, it is likely that classical cytotoxic agents will remain as cornerstones of treatment for the foreseeable future. Therefore, there is an increasing effort to optimize the use of these agents by identifying groups most likely to benefit from specific agents. Taxanes (paclitaxel and docetaxel) are commonly used in chemotherapy regimens for all stages of disease. These agents function by binding to tubulin and preventing disassembly among other mechanisms of action. High expression of specific tubulin subtypes, most notably the beta-3 isoform, has been associated with resistance to taxanes.8-10 In preclinical models, epothilones have demonstrated activity despite high 3T expression13 and are poor substrates for the multidrug resistance transporter, another potential mechanism of taxane resistance. Our trial failed to confirm the hypothesis that a regimen based on ixabepilone, the first epothilone to enter routine clinical use, would demonstrate a higher level of activity in 3T-positive disease compared with taxane-based treatment. We did prospectively confirm previous retrospective data indicating that 3T expression is an adverse prognostic and/or predictive marker for regimens containing JOURNAL OF CLINICAL ONCOLOGY Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved. Ixabepilone Plus Carboplatin in Advanced NSCLC antitubulin agents.8,19 Future studies will be needed to determine if a nonantitubulin-based regimen (eg, without taxanes, vinca alkaloids, or epothilones) can be selected based on 3T expression (ie, predictive marker) or whether 3T expression is simply an adverse prognostic marker for NSCLC. AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST Although all authors completed the disclosure declaration, the following author(s) and/or an author’s immediate family member(s) indicated a financial or other interest that is relevant to the subject matter under consideration in this article. Certain relationships marked with a “U” are those for which no compensation was received; those relationships marked with a “C” were compensated. For a detailed description of the disclosure categories, or for more information about ASCO’s conflict of interest policy, please refer to the Author Disclosure Declaration and the Disclosures of Potential Conflicts of Interest section in Information for Contributors. Employment or Leadership Position: Remigiusz Kaleta, Bristol-Myers Squibb (C); Pralay Mukhopadhyay, Bristol-Myers Squibb (C); Ovidiu C. Trifan, Bristol-Myers Squibb (C); Laura Whitaker, Bristol-Myers Squibb (C) Consultant or Advisory Role: Martin J. Edelman, Bristol-Myers Squibb (C); Elisabeth Quoix, Bristol-Myers Squibb (C); Martin Reck, Eli REFERENCES 1. Schiller JH, Harrington D, Belani CP, et al: Comparison of four chemotherapy regimens for advanced non-small cell lung cancer. N Engl J Med 346:92-98, 2002 2. Kelly K, Crowley J, Bunn PA Jr, et al: Randomized phase three trial of paclitaxel plus carboplatin versus vinorelbine plus cisplatin in the treatment of patients with advanced non–small-cell lung cancer: A Southwest Oncology Group trial. J Clin Oncol 19:3210-3218, 2001 3. Scagliotti GV, Parikh P, von Pawel J, et al: Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapynaive patients with advanced-stage non–small-cell lung cancer. J Clin Oncol 26:3543-3551, 2008 4. Sandler A, Gray R, Perry MC, et al: Paclitaxelcarboplatin alone or with bevacizumab for non-smallcell lung cancer. N Engl J Med 355:2542-2550, 2006 5. Han JY, Lim HS, Shin ES, et al: Comprehensive analysis of UGT1A polymorphisms predictive for pharmacokinetics and treatment outcome in patients with non–small-cell lung cancer treated with irinotecan and cisplatin. J Clin Oncol 24:22372244, 2006 6. Rosell R, Danenberg KD, Alberola V, et al: Ribonucleotide reductase messenger RNA expression and survival in gemcitabine/cisplatin-treated Lilly (C), F. Hoffman-La Roche (C), AstraZeneca (C), Daiichi Sankyo (C), Bristol-Myers Squibb (C) Stock Ownership: Remigiusz Kaleta, Bristol-Myers Squibb; Pralay Mukhopadhyay, Bristol-Myers Squibb; Ovidiu C. Trifan, Bristol-Myers Squibb; Laura Whitaker, Bristol-Myers Squibb Honoraria: Martin J. Edelman, Bristol-Myers Squibb; Chun-Ming Tsai, Eli Lilly, AstraZeneca, Roche, Boehringer Ingelheim, Pfizer; Martin Reck, Eli Lilly, F. Hoffman-La Roche, Daiichi Sankyo, AstraZeneca Research Funding: Martin J. Edelman, Bristol-Myers Squibb Expert Testimony: None Other Remuneration: None AUTHOR CONTRIBUTIONS Conception and design: Martin J. Edelman, Heung-Tae Kim, Pralay Mukhopadhyay, Ovidiu C. Trifan, Laura Whitaker, Martin Reck Provision of study materials or patients: Martin J. Edelman, Claude-Peter Schneider, Chun-Ming Tsai, Heung-Tae Kim, Elisabeth Quoix, Alexander V. Luft, Martin Reck Collection and assembly of data: Martin J. Edelman, Claus-Peter Schneider, Chun-Ming Tsai, Elisabeth Quoix, Remigiusz Kaleta, Ovidiu C. Trifan, Laura Whitaker, Martin Reck Data analysis and interpretation: Martin J. Edelman, Chun-Ming Tsai, Alexander V. Luft, Pralay Mukhopadhyay, Ovidiu C. Trifan, Martin Reck Manuscript writing: All authors Final approval of manuscript: All authors advanced non-small cell lung cancer patients. Clin Cancer Res 10:1318-1325, 2004 7. Se`ve P, Dumontet C: Is class III beta-tubulin a predictive factor in patients receiving tubulin-binding agents? Lancet Oncol 9:168-175, 2008 8. Se`ve P, Mackey J, Isaac S, et al: Class III beta-tubulin expression in tumor cells predicts response and outcome in patients with non-small cell lung cancer receiving paclitaxel. Mol Cancer Ther 4:2001-2007, 2005 9. Mozzetti S, Ferlini C, Concolino P, et al: Class III beta-tubulin overexpression is a prominent mechanism of paclitaxel resistance in ovarian cancer patients. Clin Cancer Res 11:298-305, 2005 10. Paradiso A, Mangia A, Chiriatti A, et al: Biomarkers predictive for clinical efficacy of taxol-based chemotherapy in advanced breast cancer. Ann Oncol 16:iv14-iv19, 2005 (suppl 4) 11. Bollag DM, McQueney PA, Zhu J, et al: Epothilones, a new class of microtubule-stabilizing agents with a taxol-like mechanism of action. Cancer Res 55:2325-2333, 1995 12. Lee FY, Borzilleri R, Fairchild CR, et al: BMS247550: A novel epothilone analog with a mode of action similar to paclitaxel but possessing superior antitumor efficacy. Clin Cancer Res 7:1429-1437, 2001 13. Lee FY, Smykla R, Johnston K, et al: Preclinical efficacy spectrum and pharmacokinetics of ixabepilone. Cancer Chemother Pharmacol 63:201212, 2009 14. Jordan MA, Miller H, Ni L, et al: The Pat-21 breast cancer model derived from a patient with primary taxol resistance recapitulates the phenotype of its origin, has altered beta-tubulin expression and is sensitive to ixabepilone. J Clin Oncol 47, 2006 (suppl; abstr LB-280) 15. Dumontet C, Jordan MA, Lee FF: Ixabepilone: Targeting betaIII-tubulin expression in taxaneresistant malignancies. Mol Cancer Ther 8:17-25, 2009 16. Vansteenkiste J, Lara PN Jr, Le Chevalier T, et al: Phase II clinical trial of the epothilone B analog, ixabepilone, in patients with non–small-cell lung cancer whose tumors have failed first-line platinumbased chemotherapy. J Clin Oncol 25:3448-3455, 2007 17. Plummer R, Woll P, Fyfe D, et al: A phase I and pharmacokinetic study of ixabepilone in combination with carboplatin in patients with advanced solid malignancies. Clin Cancer Res 14:8288-8294, 2008 18. Se`ve P, Isaac S, Tre´dan O, et al: Expression of class III -tubulin is predictive of patient outcome in patients with non-small cell lung cancer receiving vinorelbine-based chemotherapy. Clin Cancer Res 11:5481-5486, 2005 19. Reiman T, Lai R, Veillard AS, et al: Crossvalidation study of class III beta-tubulin as a predictive marker for benefit from adjuvant chemotherapy in resected non-small-cell lung cancer: Analysis of four randomized trials. Ann Oncol 23:86-93, 2012 ■ ■ ■ www.jco.org © 2013 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved. 7 Edelman et al Acknowledgment We thank patients and investigators for their participation in the trial. We also thank Sudha Vemuri, PhD, Bristol-Myers Squibb, for her writing and editorial support. The authors take full responsibility for the content of this publication and confirm that it reflects their viewpoint and scientific expertise. We also wish to acknowledge StemScientific, funded by Bristol-Myers Squibb, for providing editorial support in the preparation of this article before submission. Appendix Table A1. Summary of PFS and ORR Results 3T Positiveⴱ PFS, months Median 80% CI 95% CI Events No. % HR 80% CI One-sided 90% CI Log-rank P One sided Two sided Response rate No. % 80% CI 95% CI 3T Negativeⴱ PFS, months Median 80% CI 95% CI Events No. % HR 80% CI One-sided 90% CI Log-rank P One sided Two sided Response rate No. % 80% CI 95% CI 8 © 2013 by American Society of Clinical Oncology Ixabepilone Plus Carboplatin (n ⫽ 53) Paclitaxel Plus Carboplatin (n ⫽ 51) 4.27 3.22 to 4.90 2.89 to 5.65 4.27 4.01 to 5.42 3.61 to 6.05 42 79.2 40 78.4 1.04 0.78 to 1.41 — to 1.41 .853 .5735 9 17.0 10.5 to 25.5 8.1 to 29.8 15 29.4 21.0 to 39.1 17.5 to 43.8 Ixabepilone Plus Carboplatin (n ⫽ 45) Paclitaxel Plus Carboplatin (n ⫽ 48) 5.78 5.32 to 6.83 5.29 to 8.41 5.32 4.40 to 5.78 4.27 to 5.98 27 60.0 35 72.9 0.78 0.55 to 1.10 — to 1.10 .3500 .1750 12 26.7 18.1 to 36.9 14.6 to 41.9 (continued on following page) 13 27.1 18.7 to 37.0 15.3 to 41.8 JOURNAL OF CLINICAL ONCOLOGY Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved. Ixabepilone Plus Carboplatin in Advanced NSCLC Table A1. Summary of PFS and ORR Results (continued) Overall Population PFS, months Median 80% CI 95% CI Events No. % HR 80% CI One-sided 90% CI Log-rank P One sided Two sided Response rate No. % 80% CI 95% CI Ixabepilone Plus Carboplatin (n ⫽ 98) Paclitaxel Plus Carboplatin (n ⫽ 99) 5.29 4.27 to 5.65 4.14 to 5.88 5.13 4.27 to 5.59 4.21 to 5.78 69 70.4 75 75.8 0.92 0.73 to 1.15 — to 1.15 .632 .316 21 21.4 16.1 to 27.7 13.8 to 30.9 28 28.3 22.4 to 34.9 19.7 to 38.2 Abbreviations: 3T, beta-3 tubulin; HR, hazard ratio; ORR, overall response rate; PFS, progression-free survival. ⴱ 3T status based on internal variable region data. www.jco.org © 2013 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved. 9 Edelman et al Table A2. Summary of OS Results 3T Positiveⴱ OS, months Median 80% CI 95% CI Events No. % HR 80% CI One-sided 90% CI Log-rank P Two sided One sided 3T Negativeⴱ OS, months Median 80% CI 95% CI Events No. % HR 80% CI One-sided 90% CI Log-rank P Two sided One sided Overall Population OS, months Median 80% CI 95% CI Events No. % HR 80% CI One-sided 90% CI Log-rank P Two sided One sided Ixabepilone Plus Carboplatin (n ⫽ 53) Paclitaxel Plus Carboplatin (n ⫽ 51) 10.61 7.79 to 12.42 7.16 to 13.96 11.37 9.23 to 13.93 8.15 to 15.41 46 86.8 34 66.67 1.60 1.20 to 2.10 — to 2.10 .053 .9735 Ixabepilone Plus Carboplatin (n ⫽ 45) Paclitaxel Plus Carboplatin (n ⫽ 48) 16.92 14.26 to 23.56 13.04 to 27.96 9.40 8.25 to 12.29 7.98 to 13.40 23 51.1 34 70.8 0.70 — to 0.90 .123 .0615 Ixabepilone Plus Carboplatin (n ⫽ 98) Paclitaxel Plus Carboplatin (n ⫽ 99) 13.04 10.74 to 14.26 9.99 to 14.52 10.15 9.00 to 12.29 8.28 to 13.40 69 70.4 68 68.7 1.10 0.90 to 1.40 — to 1.40 .622 .689 Abbreviations: 3T, beta-3 tubulin; HR, hazard ratio; OS, overall survival. ⴱ 3T status is based on IVRS data 10 © 2013 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY Downloaded from jco.ascopubs.org on May 30, 2014. For personal use only. No other uses without permission. Copyright © 2013 American Society of Clinical Oncology. All rights reserved.
© Copyright 2026 ExpyDoc