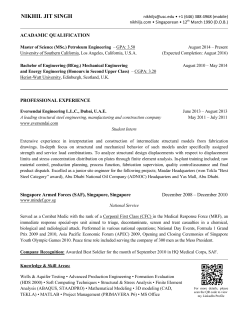
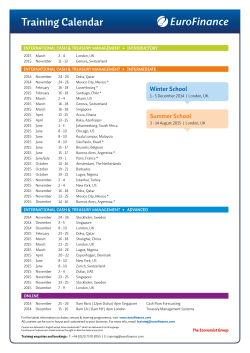
July to September 2014 Médico A quarterly publication of GP Liaison Centre, National University Hospital, Singapore. MCI(P) 151/07/2014 Medical Sp tlight Approaches to Refractory Cancers SILS in HPB Surgeries in NUH Surgical Treatment in Bone Metastases - A Changing Paradigm Associate Professor Quek Swee Tian 02-03 Medical Notes • 04-06 Medical Spotlight • 07-14 Insight • 15-17 Treatment Room • 18-21 Doctor’s Heartbeat • 22-23 Medical Notes M EDIC AL N O TES NCIS Yong Siew Yoon (YSY) Wing at the NUH Medical Centre The National University Cancer Institute, Singapore (NCIS) has come a long way since its first ambulatory oncology centre was set up in Singapore at the National University Hospital (NUH) in September 1988. Today, NCIS boasts a broad spectrum of substantial capabilities and facilities spanning over three floors from Level 8 to 10 of the all-new NUH Medical Centre, providing one-stop holistic and comprehensive care, management and treatment for both adult and paediatric oncology patients. NCIS moved most of its outpatient facilities, e.g., Breast Care Centre, Viva-University Children’s Cancer Centre, Stem Cell Therapy Centre, Chemotherapy Centre, as well as the Cancer Centre, into its current premises in the Yong Siew Yoon wing of the NUH Medical Centre in August 2013. The relocation of the Radiation Therapy Centre (RTC) from the Main Building of NUH to its new location at the new wing in February 2014 completed the move. 2 • MED ICO J ULY - se ptemb er 2 014 Figure 1. Resource Library @ Health Resource Centre Figure 2. Patient Care at Chemotherapy Centre Housed alongside other outpatient medical specialisations at the Medical Centre, NCIS brings together the expertise of multiple clinical departments to provide multidisciplinary cancer care via a convenient and accessible one-stop platform to allow for more efficient consultations and treatment processes to be carried out under one-roof. Located at high level above ground (Level 8 of the NUH Medical Centre) and with its expanded floor space of 2,500 square metres, NCIS’ relocated Radiation Therapy Centre now has an increased capacity for six linear accelerators, outpatient consultation rooms, teaching hubs, as well as CT simulation and treatment planning rooms while its new Breast Care Centre provides a comprehensive diagnosis and treatment platform for patients with various breast conditions, including imaging, surgery, preservation and reconstruction. Figure 3. Viva-University Children’s Cancer Centre Having undergone an expansion to 550 square metres (from 320 square metres), the Viva-University Children’s Cancer Centre is now able to accommodate increased capacity for oncology and bone marrow transplant therapy. Patients are also able to relax in comfort while receiving chemotherapy as the paediatric infusion bays come with inbuilt television monitors where beds are provided to the children for resting. Designed with patients’ convenience in mind, the Stem Cell Therapy Centre, Chemotherapy Centre, as well as the Pharmacy @ NCIS have also been consolidated into dedicated one-stop centres. The Cancer Centre is also strategically located on the same floor as the surgical oncology area so as to reduce travelling time on the patient front. As NCIS understands the emotional distress faced by cancer patients, a holistic approach is adopted for its treatment processes, with its new Health Resource Centre (HRC) offering support programmes and services for both adult and paediatric patients and their caregivers. Both patients and caregivers can visit its resource library stocked with over 900 titles of fiction and non-fiction books of different genres. Now, the Health Resource Centre on the 10th floor of Yong Siew Yoon wing of the NUH Medical Centre is also home to a number of cancer support groups. Lifestyle, support and educational programmes are conducted on a regular basis to promote well-being and enhance quality of life for patients and caregivers. 2 014 JULY - S E P T E M B E R M EDICO • 3 M EDIC AL S PO TLIGHT A/Prof Chng Wee Joo Director, National University Cancer Institute, Singapore (NCIS) Head and Senior Consultant, Division of Haematology, Department of Haematology-Oncology, National University Cancer Institute, Singapore (NCIS) Associate Professor Chng Wee Joo was appointed Director of NCIS on 1 September 2014. He is the Head of the Division of Haematology and a Senior Consultant at NCIS. He is also the Deputy Director of the Cancer Science Institute of Singapore at the National University of Singapore (NUS). He obtained his medical degree from the University of Leeds, UK, and did his internal medicine residency in the United Kingdom. His fellowship training in haematology was completed in Singapore before he obtained an A*STAR international fellowship in 2004 to go to the Mayo Clinic for a research fellowship in multiple myeloma genetics. His current research is very translational and involves the use of high-resolution global genomic technique to understand biology, identify drug targets, understand drug resistance and improve disease prognosis in haematological malignancies, with the ultimate aim of improving patient’s outcome and personalising treatment. Most cancers are not curable. One of the common terminal events in these incurable cancers is the refractoriness to treatment. Tumours become refractory when they become resistant to treatment. Current treatment for cancers utilises the following modalities either alone or in combination: 1) Chemotherapy which kills both cancer cells and normal cells by interfering with DNA synthesis and relying on the resulting activation of DNA damage checkpoint to kill the damage cells. 2) Radiotherapy which similarly damages DNA and affects both cancer and normal cells. 3) Targeted therapy which comes in two general forms: a. Small molecules that target enzymes and signalling molecules which are critical for the malignant potential as well as the survival of cancer cells. These molecules may be mutated or function abnormally in cancer 4 • MED ICO J ULY - se ptemb er 2 014 Approaches to Refractory Cancers cells, but not in normal cells where the cancer cells become critically dependent on them. Therefore, their inhibition by drugs will result in preferential killing of cancer cells. b. Therapeutic antibodies that bind specifically to proteins expressed on cancer cells. In most instances, these proteins are expressed at much higher level on cancer cells than normal cells. These antibodies either can directly kill the cancer cells, activate the patient’s immune system to kill the cells, or can be bound to drugs and act as a conduit to deliver the drug into the cells that they bind to. Tumours become resistant to treatment through a number of different mechanisms: 1) The tumour cells express drug transporters that pump out toxic chemotherapy so that it cannot damage the cancer cells. 2) The tumour cells develop mutations in the genes being targeted by the treatment such that the treatment is no longer able to inhibit the gene. 3) The tumour cells increase expression of the gene and protein targeted by the drugs so that the dose of drug used will not be able to inhibit all the abnormal gene or protein that is driving the cancer. 4) The tumour cells develop mutations in alternative signalling pathways such that the original target becomes no longer relevant. 5) The tumour cells develop mutations in genes that result in an ability for the tumour cells to avoid death. a tumour becomes refractory. Once we understand the mechanisms, we can design therapeutic strategies to resensitise the tumour to treatment. Another approach is to identify potential new genes, proteins or pathways in the tumour that may be important for the survival of the tumour. As these are not currently targeted by existing treatment, the tumour can escape from the effects of the existing therapy. However, if these critical pathways are targeted, the cells can still be killed. The next possible approach is to utilise different modality of treatment that is not dependent on conventional mechanisms of killing the tumour cells. Chemotherapy and radiotherapy utilise DNA damage to trigger death pathways. This requires an intact p53 protein which acts as the guardian of our genome and triggers death pathways to remove cells where the genome is damaged. The p53 gene is often mutated and not functioning in refractory cancer. For small molecular targeted therapy, the tumour cells can become refractory through a variety of mechanisms as highlighted above. Hence, using an approach that does not require p53 or signalling targets may overcome these problems. One such approach is by using immunotherapy which utilises our immune system or antibodies to kill tumour cells by specifically recognising proteins that are expressed on cancer cells. As the killing mechanisms and targets are different from chemotherapy and targeted drugs, this therapeutic modality may provide an alternative method to eradicate the cancer cells. Ways to overcome refractoriness NCIS’s approaches to refractory cancer One way to approach the problem is to identify the mechanisms through which At NCIS, we adopted the following strategies to tackle refractory tumours: 1) Expanding our Portfolio of Phase 1 Trials Over the years, we have expanded on our ability to do early phase clinical trials by building the appropriate infrastructure and clinical trial teams. Now, we have a dedicated Phase 1 clinic as well as an inpatient set-up for patients on Phase 1 clinical trials. We have also established useful partnerships and track records with some pharmaceutical companies and have an increasing portfolio of Phase 1 clinical trials (Table 1 and 2). This is an important way in providing novel therapeutic agents against new targets for patients with refractory tumours where conventional therapies have failed. 2) Genomic profiling of tumours For a better understanding of the pathways and mutations that are present in a refractory tumour, we have initiated a study where all patients with refractory cancers suitable for Phase 1 studies will have their tumours profiled using genetic sequencing (Figure 1). This will help us identify the gene mutations that may be present in these tumours. These gene mutations can potentially be targeted by new drugs being tested in Phase 1 studies and we can then match these patients to the trials. 3) Immunotherapy This area encompasses a number of different strategies that harness the patient’s own immune system to kill cancer cells. As the approach is novel and utilises non-conventional therapeutic pathways, there is a potential to overcome resistance to conventional therapy. NCIS has been active in these areas and has been developing a number of different strategies. a) Therapeutic antibodies (Figure 2) These molecules are able to recognise specific targets on cells as well as home-in to and engage with the targeted cells. Upon engagement, they can be designed to do several things. First, they can block the binding of key signalling molecule so that the pathway cannot be activated. Second, they can activate Study Title Company Total recruited A Phase 1 pharmacokinetic study of oral MLN9708 plus Lenalidomide and Dexamethasone in adult Asian patients with relapsed and/or refractory multiple myeloma Millennium 6 Phase 1 dose escalation study of oral administration of Pan-Histone Deacetylase (HDAC) inhibitor S 78454 given in combination with a fixed dose infusion of cisplatin in patients with advanced non-keratinising nasopharyngeal carcinoma Servier 3 A Phase 1b, open-label study evaluating the safety, tolerability, and pharmacokinetics of onartuzumab given as a single agent and in combination with sorafenib in patients with advanced hepatocellular carcinoma (HCC) Roche 0 An open-label Phase 1 dose-escalation study to characterise the safety, tolerability, pharmacokinetics, and maximum tolerated dose of BAY 1143572 given in a once-daily or an intermittent dosing schedule in subjects with advanced malignancies Bayer 4 Phase 1, open-label, dose escalation study of Anti-CD98 monoclonal antibody KHK2898 as monotherapy in subjects with advanced solid tumours who no longer respond to standard therapy or for whom no standard therapy is available Kyowa Hakko Kirin Co 0 An open label Phase 1 dose-escalation study to characterise the safety, tolerability, pharmacokinetics, and maximum tolerated dose of BAY 1082439 given once daily in subjects with advanced malignancies Bayer 9 Lead-In Phase 1 dose-escalating, open-label, non-randomised study of a weekly regimen OPB-51602 in advanced refractory solid tumours with enrichment cohorts of nasopharyngeal carcinoma followed by a biomarker study evaluating OPB-51602 in locally advanced nasopharyngeal carcinoma prior to definitive chemoradiotherapy NUH 2 A multi-centre, open-label study to assess pharmacokinetics of TK1258 in adult cancer patients with normal and impaired hepatic function Novartis 0 Prospective study of UDP-gluconoryltransferase (UGT) 2B17 genotype as a predictive marker of exemestane pharmacokinetics and pharmacodynamics in Asian women with hormone receptor-positive advanced breast cancer NUH 15 An investigator sponsored Phase 1 study of the saety, pharmacokinetics and pharmacodynamics of escalating doses followed by dose expansion of the Selective Inhibitor of Nuclear Export (SINE) Selinexor (KPT-330) in Asian patients with advanced or metastatic solid tumour malignancies NUH 3 42 Total Table 1. Current Phase 1 studies and recruitment Drug Class Company Type Start Date End Date Total recruited Status ABT869 VEGFR TKI Abbott First-inman Oct-06 Sep-07 45 Completed SB939 Histone deacetylase inhibitor S*Bio First-inman Apr-07 Sep-08 25 Completed OPB51602 Stat3 inhibitor Otsuka First-inman Oct-09 Jan-13 45 Completed Table 2. Completed First-in-man and First-in-class Phase 1 programs Figure 1. Schema of the IMAC study initiated at NCIS 2 014 JULY - S E P T E M B E R M EDICO • 5 Figure 2. Different ways a therapeutic antibody can be modified From a specific antibody, the sequence can be used to generate chimeric antigen receptors. Antisense gene can be encapsulated in nanoparticle that is conjugated to the antibody to achieve dual specific of targeting specific gene in specific cells that express proteins targeted by the antibody on the cell membrane. Lastly, drugs can be conjugated to the antibody which will kill the tumour cell when the antibody drug conjugate is internalised into the cells after binding. the immune system to destroy cells that they tag. Third, they can directly trigger cell death. Fourth, for some antibodies, drugs or radio-isotypes can be attached to them so that when they are internalised into the cells after engagement with the target, the target cells will be destroyed by the drug or radiation. NCIS has been working with different A*STAR research institutes - namely the Singapore Immunology Network and the Bioprocessing Technology Institute - to generate antibodies that specifically recognise cancer cells, in particular, cancer stem cells that are the source of disease relapse and usually resistant to treatment. These studies are producing exciting results when tested in cell lines and will hopefully reach the stage of human studies in the coming few years. b) Chimeric antigen receptors (CARs) These are molecular constructs that specifically recognise a target at one end and activate the immune system on the other end. These are used to modify T-cell or natural killer cells which are potent effector cells of the immune system that carry out killing functions. After modification, the T-cells or NK-cells act like armed missiles targeting cells that express the protein specifically targeted by the receptor. These CAR-T cells have been shown to have remarkable therapeutic effects in refractory acute lymphoblastic leukaemia and chronic lymphocytic leukaemia. 6 • MED ICO J ULY - se ptemb er 2 014 At NCIS, through our collaboration with one of the experts in this area, Professor Dario Campana, a professor in the Department of Paediatrics, NUS, we have initiated a clinical trial using these constructs in acute lymphoblastic leukaemia with residual disease after conventional chemotherapy. At the same time, with any promising antibodies we identify, we can use the specific recognition sequence to generate CARs. The parallel development of CARs and therapeutic antibodies allow us to quickly build a menu of therapeutics products against refractory tumours. c) Expanded natural killer (NK) cells As previously mentioned, NK cells are potent at killing certain types of tumour cells but limited by their low levels and difficulty in expanding them. Through the work of Professor Campana who has developed an effective method of expanding these NK cells, we now have a number of clinical trials using expanded NK cells against different cancers including acute myeloid leukaemia, T-cell acute lymphoblastic leukaemia, myelodysplastic, paediatric Ewing Sarcoma, and rhabdomyosarcoma. In addition, NK cells can recognise antibody bound cells and kill them. In this way, they can potentially increase the therapeutic effect of therapeutic antibodies. With the expanded NK cells, we also have other clinical trials in gastric and breast cancer, which utilise expanded NK cells together with trastuzumab, an antibody against HER2 that is overexpressed in subsets of breast and gastric cancer. These different immunotherapeutic strategies can also be used in combinations, for example, therapeutic antibodies with expanded NK cells. Targets of therapeutic antibodies can be used to generate CARs. They represent the real cutting edge of cancer therapeutics. Immunotherapy has been voted as the therapeutic breakthrough for year 2013 by Science magazine, one of the top scientific journals. And, NCIS is right at the forefront of this field with five clinical trials currently on-going. 4) Understanding mechanism of drug resistance While offering the different novel therapeutic options, we also seek to identify the mechanisms by which tumours become refractory. In particular, we studied the molecular differences between cancer stem cells, which are often refractory to cancer treatment and lead to disease relapse. Through this work, we have identified proteins that we are developing antibodies against to as well as intracellular signalling that could be targeted. In addition, we are studying the drug resistant pathways that are activated in refractory tumours and can be targeted by either existing drugs or drugs in developmental stage. We hope that these studies will lead to subsequent clinical trials that may overcome drug resistance in some types of cancers. Conclusions Tumour becomes refractory when conventional treatment fails. NCIS has developed a series of strategies and portfolio of clinical trials to target these tumours, and bring hope to patients where there is normally none. Insight A/Prof Chang Kin Yong Stephen Senior Consultant, Division of Hepatobiliary and Pancreatic Surgery, University Surgical Cluster Associate Professor Stephen Chang is currently a Senior Consultant in the Division of Hepatobiliary and Pancreatic Surgery at the National University Hospital (NUH). He is also part of the Surgical Oncology team in the National University Cancer Institute, Singapore (NCIS). He graduated with MBBS in 1994 and obtained his Master of Medicine in Surgery in 2000 from the National University of Singapore and obtained his Fellowship in Surgery from the Royal College of Surgeons of Edinburgh in 2003. He went on to further his training in Laparoscopic Hepatobiliary and Pancreatic Surgery and Liver Transplantation in Paris, France under the mentorship of Professor Daniel Cherqui before returning to Singapore in 2005. He is a key developer of the laparoscopic approach to Hepatobiliary and Pancreatic Surgery in this region and eagerly shares his skills with the other surgeons in Singapore and regionally through courses and telecommunication. He is also active in developing the Living Donor Liver Transplant Programme in Singapore. In addition, he is the pioneer of the Single Incision Laparoscopic Surgery in the region. In addition to his surgical practice, A/Prof Chang holds the appointment of Research Director in his Division and has several research interests. A/Prof Chang has also been appointed as Associate Professor at his Alumni University, NUS under the Clinician Investigator track. A/Prof Chang is actively involved in both undergraduate and postgraduate teaching and is serving as core faculty in the postgraduate General Surgery training programme. Administratively, he sits on the board of the Chapter of General Surgeons in the Academy of Medicine of Singapore. He is also the Joint Commission International Champion for the Department of General Surgery and has keen interest in improving the quality of patient care. A/Prof Chang is the current President of the Hepatopancreatobiliary Association of Singapore which is organising this year’s Liver Disease Awareness Week from 21st to 28th September 2014. The opening ceremony will be held on 21st September at the NUHS Tower Block in conjunction with NCIS’s Liver Cancer Awareness Campaign. For further details regarding the public symposium in this campaign, please visit www.ncis.com.sg or call 6772 3443. SILS in HPB Surgeries in NUH Minimally invasive surgery has revolutionised surgical techniques, and has made a huge impact in surgery. Its benefits over traditional open surgery include improved cosmesis, decreased post-operative pain, shortened length of hospital stay, and faster return to function. Surgeons all over the world have not stopped extending its application to various surgeries previously thought to be only approachable via the open surgery approach. Such boundaries have progressively been broken. More recently, the quest for minimising the abdominal wall intrusion has led to the development of single incision laparoscopic surgery (SILS). The initial interest was met with various technical difficulties. However, with adoption of new ways in handling the instruments and improved surgical techniques, interest of this potentially ‘scarless’ approach is on the rise. Since 2008, there has been increasing number of publications using this approach, and its application began to extend from the less complicated appendicectomy and cholecystectomy to the more complex colorectal and urological procedures. In NUH, since 2008, we have started performing single incision laparoscopic cholecystectomies. By early 2013, we have gained more than 300 case experiences and have since published widely in this topic, which contribute to the scientific value of this approach, including a randomised control trial on post-operative pain experience. Traditionally, hepatopancreatobiliary surgery has been the ‘holy grail’ of all abdominal surgery. But, in the last decade, many major hepatobiliary surgeries have been performed with the laparoscopic approach. In NUH, we have started performing some of these complex hepatobiliary surgeries through the laparoscopic approach since 2005. By 2011, we have gained more than 100 case experiences in laparoscopic hepatectomies, distal pancreatectomies, and cystogastrostomy. Combining the skills gained through these laparoscopic procedures and SILS cholecystectomies, we are among the first in the world to perform complex hepatopancreatobiliary procedures via the SILS approach. SILS cholecystectomy SILS cholecystectomy was first performed in NUH in 2008. After having performed the first 30 cases, we conducted a casecontrol analysis with the conventional 4-port approach and found encouraging results1. We went on to confirm its safety and feasibility via a prospective study of the first 100 patients. The outcome of these patients was encouraging and the result was published in 20122. Subsequent to that, with funding from Covidien, we embarked on a randomised control trial, to study the pain experience in detail. We have since completed the study, and the interim report was published in September 20123. Much progress has been made in the technique of SILS cholecystectomy. In the beginning, three reusable ports were inserted through three separate fascia punctures within a single incision in the umbilicus. This technique allows the scars to be hidden within the umbilicus but the closure of these fascia openings was challenging. In early 2009, we use the first commercially fabricated SILS port device. With such device, we could then 2 014 JULY - S E P T E M B E R M EDICO • 7 References 1) Chang S, Tay CW, Bicol R, Lee YY, Madhavan K. A Case-control Study of Single-incision vs Standard Laparoscopic Cholecystectomy. World J Surg. 2011 Feb; 35(2):289-93.Chang SKY, Tan SSY, Kok YO. Early experience in single-site laparoscopic cholecystectomy. Singapore Med J 2012;53(6):377 2) Chang SK, Wang YL, Shen L, Iyer SG, Shaik AB, Lomanto D. Interim report: A randomized controlled trial comparing postoperative pain in single-incision laparoscopic cholecystectomy and conventional laparoscopic cholecystectomy. Asian J Endosc Surg. 2012 Sep 14. doi: 10.1111/j.1758-5910.2012.00154.x 3) Chang SK, Mayasari M, Ganpathi lS, Wen VL, Madhavan K. Single Port Laparoscopic Liver Resection for Hepatocellular Carcinoma: A Preliminary Report. International Journal of Hepatology. 2011;2011:579203. doi:10.4061/2011/579203 Figure 1. SILS surgery device perform the surgery through a single fascia opening which can be closed easily. Further experience in this procedure allows us to innovate in the way the tools are handled to ensure safety of the procedure. By early 2013, we have gained more than 300 case experiences in SILS cholecystectomy. Furthermore, we have been among the forerunners in sharing this experience with other surgeons at various regional and international conferences. This large experience provides us with the confidence to pioneer single incision laparoscopic surgery in other HPB surgeries, such as for liver resection and pancreas resection. SILS hepatectomy Our first SILS hepatectomy was performed in early 2010. In 2011, we reported our first three cases of SILS hepatectomies in patients with hepatocellular carcinoma in the International Journal of Hepatology4. 8 • MED ICO J ULY - se ptemb er 2 014 SILS spleen preserving distal pancreatectomy In 2011, we performed our first case of SILS spleen preserving distal pancreatectomy, and the technique was published in 20125. We find the approach to this type of surgery particularly attractive as the pancreatic specimen can be delivered through the umbilical incision fully due to its slender long shape. This leaves behind a scar well hidden in the umbilicus which in essence, no obvious scar is seen on the abdomen. Conclusion As an academic health system, we continue to strive to improve how we manage our patients and aim to be at the forefront of surgical advancement. We are thankful to be among the first few centres in the world to adopt the single incision laparoscopic approach to various hepatobiliary procedures, and we aspire to seek greater heights in the future. 4) Stephen K. Y. Chang, Davide Lomanto, Maria Mayasari. Single-Port Laparoscopic Spleen Preserving Distal Pancreatectomy. Minim Invasive Surg, 2012;2012:197429. Epub 2012 Feb 26 Insight Dr Johann Tang Senior Consultant, Department of Radiation Oncology, National University Cancer Institute, Singapore (NCIS) Dr Johann Tang, MBBS, FRANZCR, is currently a Senior Consultant at the Department of Radiation Oncology at the National University Cancer Institute Singapore (NCIS). He is also an Assistant Professor at the National University Hospital as well as Assistant Professor at the Yong Loo Lin School of Medicine, National University Singapore. After obtaining his fellowship from the Royal Australian College of Radiologist (FRANZCR), Dr Tang underwent breast brachytherapy fellowship at University of Wisconsin as well as prostate brachytherapy and paediatric fellowships at Peter Maccallum Cancer Institute, Australia. Dr Tang’s subspecialty and main research interest include breast, gynaecological, paediatrics and CNS tumours. Dr Tang set up and currently heads the breast brachytherapy and paediatric radiotherapy service. He is passionately involved in education and is currently the co-chair of the Euro Asia Breast Brachytherapy School, part of the teaching faculty of the Australian Paediatric Radiation Oncology Group and was an external examiner in radiation oncology to the Bangladesh College of Physicians and Surgeons. Besides being the Research Director for his department, Dr Tang actively mentors residents, publishes medical journals and is a referee for several international journals. Dr Tang has won several research prizes and is currently holding several research grants. He currently serves on national committees such as the Vice President of the Chapter of Radiation Oncologist, Academy of Medicine Singapore and Executive Member of the Singapore Society of Oncology. Accelerated Partial Breast Irradiation: Treating Less is Better - A New Paradigm Shift for Early Stage Breast Cancer Treatment In patients with early stage breast cancer and post breast conserving surgery cases, adjuvant radiotherapy remains as the standard of care resulting in local control as well as overall survival benefit 1 2 3 . The use of mammographic screening has enabled identification of patients with early stage breast cancer earlier, thus increasing the breast conservation rates in this group of patients4. However, the use of conventional fractionation radiotherapy which was usually given over 5 to 6 weeks may pose a barrier to patients who are receiving adjuvant radiotherapy, which later may lead to some patients opting for total mastectomy instead5.To avoid unnecessary total mastectomies, Accelerated Partial Breast Irradiation (APBI) presents a viable alternative radiotherapy modality to patients with early stage, node negative breast cancer, considering its shorter overall treatment duration. BRACHYTHERAPY COMPARED TO EXTERNAL BEAM RADIOTHERAPY Features HDR Brachytherapy External Beam Therapy Treatment areas Tumour site with margins only Entire breast Number of treatments 10 treatments over 1 week 25-30 treatments over 5-6 weeks Convenience More convenient for those with busy work schedules or long commutes Great time commitment required. May be disruptive to work schedules Radiation to adjacent organs Less radiation to lung, heart, rib and lymphatic Acceptable radiation to lung, heart, ribs and lymphatic Skin care Requires bandaging and care of catheter sites Daily application of creams during radiotherapy and about 3 months after radiotherapy Cure rates Comparable long term results to external beam radiotherapy Currently the gold standard for breast treatment Appearance Favourable cosmesis, minimal scarring Acceptable and favourable in most instances Invasive Yes, requires insertion of catheters into the breast No. External X-rays only Table 1. Pros and cons of multi-catheter APBI if being compared with a standard external beam radiotherapy 2 014 JULY - S E P T E M B E R M EDICO • 9 Insight Dr Shaik Buhari Senior Consultant, Department of General Surgery, University Surgical Cluster Type of APBI Modality His main area of expertise is breast surgery and surgical oncology, with special interest in oncoplastic and reconstructive surgery. He has had numerous presentations, at both local and international meetings, as well as publications. He has been an invited speaker at many local and regional congresses. - Recent clinical phase 3 data shows that multi-catheter APBI is equivalent to a standard EBRT treatment. - Most versatile of all the APBI modalities. - Suitable for patients of all cup sizes. - Can be used in patients with augmented breast implants. -Invasive. - Operator dependent procedure. MammoSite - Phase 2 registry data shows no inferiority to standard EBRT treatment. - Simple to insert and can be done in the surgical rooms. - Higher toxicity rates compared to multi-catheter interstitial. - Restricted to breasts with cup C size and above as the smallest diameter of the balloon catheter is 5cm. Thus, it is not suitable for majority of the Asian patients. Intra-operative radiotherapy with electrons (ELIOT) Dr Shaik Buhari is also involved in several research projects in collaboration with radiation and medical oncology. On the teaching front, he is a lecturer at the Yong Loo Lin School of Medicine, NUS and School of Nursing, NYP. He is also an examiner at the MBBS Examination in NUS. At the national level, he was in the Panel of Complaint Committee (SMC) and Reviewer for the Combined Surgical Meeting (CSM). He sits on the JCI Steering Committee, Tissue Audit Committee and Blood Bank Committee for NUH. Apart from his academic achievements, he has also been nominated for the Star Award and National Excellent Service Award (Gold). Cons Multi-catheter APBI Senior Consultant, Division of Surgical Oncology, National University Cancer Institute, Singapore (NCIS) Dr Shaik Buhari graduated from NUS in 1988. He obtained FRCSEd and M.Med (Surgery) in 1993 and was appointed as a consultant at the Department of Surgery in 2000. He worked in Nottingham Breast Institute from 2002 to 2004, where he received advanced training in breast surgery and oncoplastic surgery. Pros - Treatment is done at the time of breast conserving surgery. - Phase 3 clinical data shows higher recurrence rates compared with standard EBRT treatment. - IORT ELIOT has fallen out of favour. Targeted intra-operative radiotherapy (TARGIT) - Treatment is done at the time of breast conserving surgery. - Phase 3 clinical data shows higher recurrence rates compared with standard EBRT treatment. - IORT TARGIT has fallen out of favour. - In addition, 1 in 4 post TARGIT patients will require standard EBRT due to poor pathological features. - Not suitable for Asians due to the large electron sphere that needs to be inserted into the breasts, similar to MammoSite. APBI – External Beam - Non invasive - Suitable for any breast size. - Clinical studies have shown APBI External Beam to have higher long-term toxicity rates. Table 2. Various types of APBI modalities available This would reduce the logistic barriers, especially for those who are active in the workforce and find it difficult to take time off from work or need to travel long distances for their radiotherapy treatments. 10 • MED I CO J ULY - se ptemb er 2 014 Thus, APBI serves as a viable alternative breast conservation treatment for patients who would otherwise have opted for total mastectomies. Furthermore, where acute and late toxicities such as radiation dermatitis, acute pneumonitis and skin fibrosis are common with conventional external beam treatment, APBI offers better toxicity outcome leading to favourable cosmesis with lesser acute and late toxicity. Table 1 summarises the pros and cons of APBI versus a standard 6-week external beam treatment. Types of APBI modalities There are many different APBI modalities, e.g., intraoperative, MammoSite, multi-catheter, and external beam 6 7 8 (Figure 1). Each of these different APBI modalities has its pros and cons. Given the recent published data for various APBI techniques, it has emerged that multi-catheter APBI offers the best clinical evidence for efficacy with better toxicity profile if being compared with a standard conventional external beam radiotherapy treatment. Table 2 summarises the various types of APBI modalities available. APBI% Conventional EBRT% Figure 1. APBI versus conventional EBRT Criteria ABS ESTRO+ ASTRO+ What is multi-catheter APBI? Age ≥ 50 years old ≥ 40 years old ≥ 50 years old Amongst all the APBI modalities, multicatheter interstitial APBI is the oldest method, hence has the longest clinical follow-up and experience. Given that the area of highest risk of local recurrence involves the tumour cavity plus a 1.5 to 2-cm margin, targeting and delivering high doses of radiation to this high risk volume decreases the chance of a local recurrence. Radiation delivery is achieved by placing plastic catheters surrounding the tumour cavity. This allows the dose delivery to be highly conformal to the high risk volume, concentrating the high dose to this region, whilst sparing the surrounding organs at risk such as the normal breast tissue, ribs, lungs, and heart. This would lead to lower long-term toxicity on these organs at risk. Contrast to EBRT treatment where the dose enters the breast externally and penetrates all tissues in its path before exiting on the opposite side, all the normal tissues irradiated would be subjected to longterm toxicity. These EBRT side effects include radiation dermatitis, cardiac toxicity and pulmonary fibrosis, whereas these side effects are seldom seen in patients who have undergone multicatheter APBI. Size ≤ 3 cm ≤ 3 cm ≤ 3 cm All invasive subtypes and DCIS* All invasive subtypes and DCIS* All invasive subtypes and DCIS* Positive/Negative Positive/Negative Positive/Negative Surgical Margins Negative Negative/Close < 2 mm) Negative/Close < 2 mm) Lymphovascular Space Invasion Negative Negative Negative/Focal Nodal Status Negative < 4 Lymph Nodes Involved Negative Histology Estrogen Receptor Table 3. Summary of the study results published by the American Society for Therapeutic Radiation Oncology (ASTRO), American Brachytherapy Society (ABS), and European Society for Therapeutic Radiation Oncology (ESTRO) Who are the eligible patients? Whilst older studies using multicatheter interstitial APBI did not achieve good results which might be due to poor patient selection, recent studies have demonstrated that with careful patient selection, good clinical results and local control can be achieved with this technique9. The results of the recent studies form the basis of consensus guidelines published by the American Society for Therapeutic Radiation Oncology (ASTRO)10, American Brachytherapy Society (ABS)11, and European Society for Therapeutic Radiation Oncology (ESTRO)12, indicating which patients are suitable for multicatheter APBI, which group of the patients shall be offered with caution, and which ones of them are not suitable for the procedure. In general, the suitable and cautionary patients can be offered this procedure. At the National University Cancer Institute Singapore (NCIS), these two groups of patients make up about 80% of the total cases seen. Our experience at NCIS have shown that post breast conserving surgery patients who are above 40 years old and diagnosed with early stage breast cancer have shown to be suitable candidates for APBI. 2 014 JULY - S E P T E MB E R M EDICO • 11 Friday 9:00 – 10:00 am Catheter placement with local anaesthetic 10:30 am Breast CT stimulation Break Weekend The Following Monday to Friday Bid fractions HDR treatments, 6 hours apart No CT required before each fraction Table 4. Sample of APBI planning & treatment schedule Figure 2. Tumour cavity shown by seroma and clips Multi-catheter APBI treatment schedule location of the tumour in respect to the nipple and the depth of the normal breast tissue so as to avoid the risk of a pneumothorax by puncturing the underlying ipsilateral lung. Under local anaesthesia, implantation of the catheters usually takes place on a Friday morning and lasts for one hour. Immediately post implantation, the patient will undergo a planning CT scan and then be discharged. The treatment commences from Monday to Friday on the following week, 2 sessions a day (i.e. morning and afternoon). After the Friday treatment session, the catheters are removed. Multi-catheter APBI technique Target localisation Ultrasound guided localisation of the target is essential to a successful implant. Under ultrasound guidance, about 0.5-1 cc of omnipaque is injected into the tumour cavity. This is to allow the tumour cavity to be easily identifiable on the pre-procedure CT scan. In addition, instead of using a skin surface marker pen, the outline of the cavity is marked by imprinting the straw on the breast skin surface as the marker pen can be accidentally washed off easily when the area is cleaned with chlorhexidine solution before the procedure. By imprinting the straw marks on the skin, the impression of the cavity outline remains even after the cleaning of the ipsilateral breast preprocedure. By placing contrast into the seroma cavity, it is easier to see on the pre-procedure CT scan. Pre-procedure CT scan is then acquired to gain information on the 12 • ME D ICO J ULY - se ptemb er 2 014 Before the procedure, it is advisable to mark out the outline of medial borders of the brassiere against the bra. This is to ensure that no catheters are placed medially to this line such that it may be seen when the patient wears a low cut revealing dress. By doing this, it also ensures that patients are more confident of continuing their activities of daily living by having the freedom of what to wear and yet able to continue treatment. Figure 3. Marking out the bra line such that no catheters are placed superiorly to achieve favourable cosmesis outcomes Anaesthesia Moderate sedation is usually the mode of anaesthesia. A cocktail of Oxycodone 5 mg capsule, Valium 5 mg and Synflex 550 mg is given to the patient 45 minutes before the commencement of the procedure. Tumescence anaesthesia made up of 2% lignocaine, 1:80,000 adrenaline, sodium bicarbonate mixed in 250 ml of normal saline is used as a breast local anaesthetic agent. Other equipment includes a pair of 20 ml syringes with 11 G spinal needle attached for the delivery of the tumescence anaesthesia. Procedure The template approach is most suitable for patients with B to D cup size breast due to the use of Kuske Template size. Once the cavity is localised, the ipsilateral breast area is surgically prepped under sterile conditions. To avoid injury of the underlying chest wall structures or causing a pneumothorax, the overlying breast is pinched and gently lifted off the chest wall before applying the template and securing it. Also to note is that the C12 grid position ideally should be in the centre of the tumour cavity to ensure that adequate grid space is available on either side of the template for catheter insertion. Usually, four anchoring needles are then placed in an asymmetric pattern at C8, 12, 14 and A13. The purpose of the asymmetric pattern is to aid easy orientation of the template in reference to the patient’s anatomy as well as to secure and prevent slipping of the template from the breast. In general, any catheter within the PTV-Eval needs to be inserted. For the catheters out of the PTV-Eval, if they are within 1 cm of the PTVEval contour, they would need to be inserted as well. By using this method, one can easily determine the exact number of catheters required to cover the PTV-Eval volume and avoid under or over insertion of catheters. For cosmetic reason, it is worthwhile to avoid placing catheters outside of the patient’s low cut dress neckline so that the catheters cannot be seen when a low cut dress is worn. If the catheters protrude out into the neckline area, the best recommended measure is to manually reside the entry point of the catheter to below the neckline without compromising the dosimetric coverage. Figure 4. Diagram showing the various volumes A CT scan is then obtained with the anchoring catheters in-situ. These images are then reconstructed on the Oncentra planning system (Nucletron Elekta, Netherlands). The images are then reoriented in Oncentra to depict the “template view”. This template view is crucial in determining where the rest of the catheters should be placed. Next, an overlying photocopy of the template on a transparency is placed on the top of the screen and the “template view” template magnification is matched 1:1 to the overlaid template transparency. The corresponding anchoring needle positions are then marked on the overlaid transparency. Similar to the previous step, PTV-Eval contour and the chest wall contour are also outlined to the transparency. Once done, the rest of the catheter placement can be easily determined. Once the catheters are placed, they are then replaced with plastic catheters to ensure patient’s comfort. The blind end is flushed to the skin while the other end is trimmed to size. A numbered button is then heat-sealed to secure the other end of the catheter. Treatment delivery of the radioactive 192-Iridium source is via an after-loader machine which is remotely controlled. On the day of the treatment, the patient’s catheters are connected to the after-loader using special tubes. This is a safety mechanism to ensure that there is no chance that the radioactive source may be left in the patient. Contrary to popular belief, as the radioactive source is never in the patient, the patient is not radioactive and is free to carry babies or be around pregnant women. Figure 5. Overlaying a transparency and tracing out the various important structures to Figure 6. Kuske Template with the anchoring catheter needles in-situ aid catheter placement 2 014 JULY - S E P T E MB E R M EDICO • 13 References 1) Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011 Nov 12;378(9804):1707-16. Figure 7. Replacing the needle catheters with plastic comfort catheters Figure 8. Final appearance of the implanted breast catheters Multi-catheter APBI offers favourable longterm cosmetic results with little residual evidence of catheter implantation. Unlike EBRT treatment where there is about 5% chance of long-term skin pigmentation and fibrosis from radiation skin fibrosis, patients with multi-catheter APBI do not experience this, which may result in higher patient satisfaction. Conclusion Special advantages of multi-catheter APBI Augmented breast implant patients For patients with augmented breast implants and are diagnosed with early stage breast cancer, mastectomy is currently the only option. Having mastectomy would defeat their purpose of undergoing augmentation in the first place as majority of the patients would want to retain their breasts for various reasons. Multi-catheter APBI now offers this group of patients the chance of breast conserving treatment, allowing them to undergo adjuvant radiotherapy, conserving their breast, and avoiding a mastectomy. Done under image guidance, the chance of puncturing the breast implants using the multi-catheter APBI template technique will be low. In contrast, EBRT cannot achieve such conformal dose distribution, leading to contracture of the silicone capsule and skin fibrosis from the radiation dermatitis. 14 • MED I CO J ULY - se ptemb er 2 014 There is a new paradigm shift for a shorter yet effective radiotherapy treatment for early stage breast cancer. In selected patients, multi-catheter APBI is an effective alternative to conventional EBRT treatment, offering shorter overall treatment duration of five days, equivalent efficacy, and yet offering better toxicity profile. Increasing both physicians’ and patients’ awareness of such treatment options would thus lead to more informed decisions and better patient overall satisfaction about their treatment choice without compromising on treatment outcomes. At NCIS, multi-catheter APBI has been offered to selected patients with early stage breast cancer since 2007 with favourable clinical outcomes comparable to major American and European centres. What the physician can expect As a referring physician, you can be rest assured that NCIS will work closely with you in providing your patients with the finest treatment and continuing care possible. We will keep you well informed on the patients’ investigation results and treatment progress. Last but not least, we respect and value your knowledge of and relationship with the patients, and treasure your partnership in caring for the patients. 2)Recht A, Solin LJ. Breast -conserving surgery and radiotherapy in early-stage breast cancer: the importance of local control. Semin Radiat Oncol. 2011 Jan;21(1):3-9 3) CVinh-Hung V, Verschraegen C. Breast-conserving surgery with or without radiotherapy: pooled-analysis for risks of ipsilateral breast tumor recurrence and mortality. J Natl Cancer Inst. 2004 Jan 21;96(2):115-21 4) Olsen O, Gøtzsche PC. Screening for breast cancer with mammography. Cochrane Database Syst Rev. 2001;(4):CD001877 5) Boscoe FP, Johnson CJ, Henry KA, et al. Geographic proximity to treatment for early stage breast cancer and likelihood of mastectomy. Breast. 2011 Aug;20(4):324-8 6) Vicini FA, Arthur DW. Breast brachytherapy: North American experience. Semin Radiat Oncol. 2005 Apr;15(2):108-15. Review 7)Polgár C, Major T. Current status and perspectives of brachytherapy for breast cancer. Int J Clin Oncol. 2009 Feb;14(1):7-24 8) Skowronek J, Wawrzyniak-Hojczyk M, Ambrochowicz K. Brachytherapy in accelerated partial breast irradiation (APBI) - review of treatment methods. J Contemp Brachytherapy. 2012 Sep;4(3):152-64 9) David E. Wazer, Douglas W. Arthur, Frank A. Vicini. Accelerated Partial Breast Irradiation. 2nd Ed. Springer, 2006. p207-345 10) Smith BD, Arthur DW, Buchholz TA, et al. Accelerated partial breast irradiation consensus statement from the American Society for Radiation Oncology (ASTRO). Int J Radiat Oncol Biol Phys. 2009;74:987–1001 11) Shah C, Vicini F, Wazer DE, et al. The American Brachytherapy Society consensus statement for accelerated partial breast irradiation. Brachytherapy. 2013 Jul-Aug;12(4):267-77 12) Polgar C, Van Limbergen E, Potter R, et al. Patient selection for accelerated partial-breast irradiation (APBI) after breast conserving surgery: Recommendations of the Groupe Europeen de Curietherapie-European Society for Therapeutic Radiology and Oncology (GEC-ESTRO) breast cancer working group based on clinical evidence (2009). Radiother Oncol. 2010;94:264–273 Treatment Room Dr Gurpal Singh Consultant, Division of Musculoskeletal Oncology & Division of Hip & Knee Surgery, University Orthopaedics, Hand and Reconstructive Microsurgery Cluster Dr Gurpal Singh is a fellowship-trained Orthopaedic surgeon specialising in musculoskeletal oncology and total joint replacement in the National University Hospital (NUH). He is also part of the Musculoskeletal Cancer Group in the National University Cancer Institute, Singapore (NCIS). Dr Singh’s clinical practice consists of musculoskeletal tumours (benign, malignant and metastatic bone disease) with a focus on endoprosthetic reconstruction and limb salvage surgery, as well as primary and revision joint replacement. His academic interests include osteolysis, periprosthetic tissue responses to wear debris from failed joint replacements, infections and biomaterials in joint replacement. Dr Singh collaborates internationally with a team of musculoskeletal oncologists, arthroplasty surgeons and material scientists from Germany in an effort to continuously improve biomaterials and increase the lifespan of artificial joint prostheses, reduce infection rates and minimise adverse tissue responses from the patient’s body. Surgical Treatment of Bone Metastases – A Changing Paradigm this article is to review the principles of treatment of bone metastases and the philosophies of surgical treatment in these patients. Mechanism of cancer spread to bone Tumour cells from the primary organ site travel through the blood stream and lymphatic system to the axial and appendicular skeleton. Roodman et al. have reviewed the biology of the osteoclast and the pathophysiology of bone metastases3. The hypothesis for development of bone metastases is an interaction between tumour and bone cells causing increased bone destruction and proliferation of tumour cells within the bone marrow. Bone marrow secretes cytokines that can attract tumour cells. Introduction Bone metastasis may be defined as cancer that spreads from a primary organ site to the axial and/or appendicular skeleton. With increasing survival of cancer patients and advancement in treatment modalities, bone metastases are contributing to significant morbidity. In a recent report, it was estimated that 280,000 adults in the United States were living with metastatic bone disease with 68% of cases occurring in patients with primary breast, prostate, or lung cancer1, 2. Current decisionmaking in surgical treatment of bone metastases needs to consider both survivorship and quality of life. The main aim of the surgery is a longlasting reconstruction which outlives the patient. The aim of Figure 1. A “vicious, self-perpetuating cycle” between tumour cells and bone marrow leading to development of extensive bone metastases Local production of osteolytic factors by cancer cells in the bone stimulates osteoclast-mediated bone resorption. A “vicious, self-perpetuating cycle” between tumour cells and bone marrow leads to development of extensive bone metastases4-7. (Figure 1) Clinical presentation Patients generally present with severe bone pain; this pain is present at rest and is non-mechanical in nature. There may be night pain and poor response to conventional first-line analgesics. Patients may present with pathologic fractures (fractures occurring with trivial or no injury) or impending pathologic fractures, particularly in the lower limb. Patients may also present with neurological weakness in the lower limb and loss of bowel and bladder control due to metastases to the spine and consequent spinal cord or cauda equina compression. Spinal cord compression due to vertebral collapse caused by bone metastases is an emergency that can lead to permanent damage to the spinal cord and paralysis. Bone metastases may also present as hypercalcemia of malignancy. Table 1 shows the percentage of bone metastases from common primary organ sites1-8. Cancer of Primary organ site Bone Metastatic involvement (%) Lung 4% Gastric 9% Colorectal 13% Prostate 25% Pancreas 28% Liver 31% Breast 33% Renal 66% Table 1. The percentage of bone metastases from common primary organ sites 2 014 JULY - S E P T E MB E R M EDICO • 15 Investigations The following investigations may be performed: 1. Plain radiograph of affected bone: May show osteolytic lesions, osteoblastic lesions, and/or pathological fracture. 2. Bone scan: May show increased uptake in areas of bone metastasis. It helps to detect extent of cancer spread to the entire skeleton. 3. MRI of affected bone: To determine intramedullary extent of bone metastases and “skip” lesions. 4. CT scan of thorax, abdomen and pelvis: Helps to detect the primary organ of cancer, and may be useful in staging of disease. 5. Blood investigations: Alkaline phosphatase, calcium levels, and tumour markers where necessary. 6. Biopsy: For histopathological diagnosis. This may sometimes be performed at the time of surgical fixation. Management of bone metastasis Treatment is best undertaken in a tertiary centre involving a multi-disciplinary approach comprising the musculoskeletal oncology surgeon, medical oncologist, radiation oncologist, radiologist, advanced practice nurse, and individual specialist’s inputs depending on the nature of primary cancer. The treatment depends on whether the skeletal metastasis is solitary or multiple, the presence of visceral involvement and type of primary cancer, as well as the prognosis and general condition of the patient. Metastatic destruction of bone reduces its weight bearing capabilities, resulting initially in trabecular disruption and microfractures, and subsequently total loss of bone integrity. Principles of treatment of bone metastases include (Figure 2): I. Diagnosis and treatment of the primary cancer : In conjunction with oncologist. II.Treatment of: 1.Pain: Analgesics in conjunction with palliative medicine specialist/pain specialist, radiation therapy where appropriate. 2.Pathological fractures: Fracture fixation and/or joint replacement surgery. 16 • MED ICO J ULY - se ptemb er 2 014 3.Spinal cord compression: Spine decompression and stabilisation. 4.Impending pathological fracture: Prophylactic fracture fixation surgery where indicated. 5. Hypercalcemia. Medical management Medical treatment options for patients with bone metastases include chemotherapy, endocrine therapy, bisphosphonates, radiotherapy and pain management4-8. Chemotherapy uses combinations of drugs to destroy cancer cells. Endocrine therapy or hormone therapy is used for treatment of breast cancer and prostate cancer. Bisphosphonates may prevent or delay the development of skeletal metastases and retard bone resorption. Pain management may be difficult and best undertaken in conjunction with a palliative care physician and pain specialist. Radiotherapy is an effective modality for treatment of bone metastases 4-6, 8 in certain types of cancers. The probable mechanism of radiotherapy is radiationinduced hypoxia and death of tumour cells. This leads to local control of bone metastases and pain relief. Figure 2. Pelvic bone and hip metastases (impending fracture) Surgical management In general, surgical treatment for bone metastases consists of fracture fixation and/or resection of metastases and reconstruction of the affected bone segmental in combination with joint replacement surgeries4. These procedures help with pain relief, ambulation of the patient, and ease to carry activities of daily living. The indications of prophylactic fracture fixation include impending fracture, severe pain, and involvement of one-half or more of the cortex of the bone. Spinal cord compression from tumour metastasis to the spine and epidural space may result in permanent neurological damage unless emergency measures are undertaken to decompress the neurological structures. These patients are treated with surgical decompression of spine and stabilisation of the spine with plates and screws. Options for surgical management of metastases to the appendicular skeleton include osteosynthesis (fixation with an intramedullary nail or strong plate, in combination with adjuvants such as bone cement), endoprostheses (joint replacement prostheses), or tumour endoprostheses (modular or non-modular References Figure 3. Pelvic bone reconstruction and hip replacement components). Conventional orthopedic teaching has advocated osteosynthesis for surgical palliation of the cancer patient with bone metastases. But, recent advances in musculoskeletal oncology question the validity of this statement in today’s context of multimodal cancer care and increased survival. tumour resection (particularly for solitary metastases) and reconstruction with longer-lasting options10,11. The line between palliative and curative intent has also shifted, and the approach to a patient with a visceral malignancy and solitary metastases is often curative. Surgical palliation in metastatic bone disease has conventionally been osteosynthesis with a strong construct such as an intramedullary nail. Ideally, the construct should outlive the patient; surgery should provide effective and fast pain relief and ambulation and there should be an improvement in survival after surgery, particularly for solitary metastases9. Perhaps, the final issue that deserves to be mentioned is the cost-effectiveness of surgical treatment of bone metastases, and as a subset, the justification of increased cost of treating bone metastases with tumour endoprostheses. Skeletal related events (SRE’s) from bone metastatic disease result in significant health resource utilisation and impose a substantial financial burden on health systems. Treatments that delay or prevent SRE’s therefore result in considerable cost-savings12. We have shown that it is more cost-effective to surgically reconstruct metastases around the hip joint in appropriately selected patients, as compared to the costs of conservatively managing these patients in a step-down care facility in the Singapore context13. With increased survival of patients with long bone metastases, tumour recurrence, failure of the osteosynthesis construct and continuing pain are increasing in incidence. Thus, the idea of the osteosynthetic construct surviving the patient may not be able to keep up with the rapid advances in multimodal treatments which allow patients with bone metastases to live much longer. There has been a frameshift in thinking with regards to optimal surgical management of patients with metastases, with a greater emphasis on Ashford et al, 2010,14 reviewed the financial implications of using proximal femoral replacements for metastatic bone disease and reported that in their setting, endoprosthetic replacements were found as an effective treatment but poorly reimbursed under their funding arrangements. Thus, cost remains a concern, and funding arrangements differ from country to country. In appropriately selected patients, the benefits of resection of bone metastases and appropriate reconstruction probably outweigh the increased cost. 1) Shuling Li, Yi Peng, Eric D Weinhandl, Anne H Blaes,Karynsa Cetin, Victoria M Chia, et al, Estimated number of prevalent cases of metastatic bone disease in the US adult population Clin Epidemiol. 2012; 4: 87–93 2) Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ: Cancer statistics, 2009.CA Cancer J Clin 2009 ; 59(4):225-49 3) Teramachi J1, Zhou H, Subler MA, Kitagawa Y, Galson DL, Roodman et al. Increased IL-6 Expression in Osteoclasts Is Necessary But Not Sufficient for the Development of Paget’s Disease of Bone. J Bone Miner Res. 2014 Jun; 29(6):1456-65. 4) Harrington KD. Orthopedic surgical management of skeletal complications of malignancy Cancer. 1997;80:1614-27 5) Yazawa Y, Frassica FJ, Chao EY, et al. Metastatic bone disease. A study of the surgical treatment of 166 pathologic humeral and femoral fractures. Clin Orthop Relat Res. 1990 (251):213-9 6) Nieder C. Repeat palliative radiotherapy for painful bone metastases. Lancet Oncol. Lancet Oncol. 2014 Feb; 15(2):126-8 7) Barrett-Lee P, Casbard A, Abraham J, Hood K, Coleman R, Simmonds P, et al. Oral ibandronic acid versus intravenous zoledronic acid in treatment of bone metastases from breast cancer: a randomised, open label, non-inferiority phase 3 trial. Lancet Oncol. Jan 2014;15(1):114-22 8) Howard A Chansky .Metastatic Bone Disease. Medscape Medical News 9) Attar S, Steffner RJ, Avedian R, Hussain WM. Surgical intervention of nonvertebral osseous metastasis. Cancer Control 2012;19:113-121 10) Harvey N, Ahlmann ER, Allison DC, Wang L, Menendez LR. Endoprostheses last longer than intramedullary devices in proximal femur metastases. Clin Orthop Relat Res 2012;470:684-691 11) Wedin R, Bauer HC. Surgical treatment of skeletal metastatic lesions of the proximal femur: endoprosthesis or reconstruction nail? The Journal of bone and Joint surgery British volume 2005;87:16531657 12) Hechmati G, Cure S, Gouépo A, Hoefeler H, Lorusso V, Lüftner D, Duran I, Garzon-Rodriguez C, Ashcroft J, Wei R, Ghelani P, Bahl A.Cost of skeletal-related events in European patients with solid tumours and bone metastases: data from a prospective multinational observational study. J Med Econ. 2013;16(5):691-700 13) Singh G, Lim CT, Jonathan TJ, Nathan SS. Evaluation of the role and costeffectiveness of end-of-life orthopaedic interventions in cancer patients with skeletal metastases to the hip. J Palliat Care. 2013 Summer;29(2):83-90 14) Ashford RU, Hanna SA, Park DH, Pollock RC, Skinner JA, Briggs TW, Cannon SR. Proximal femoral replacements for metastatic bone disease: financial implications for sarcoma units. Int Orthop. 2010 Jun;34(5):709-13 2 014 JULY - S E P T E MB E R M EDICO • 17 D OCT OR’S H EAR TBEAT A/Prof Quek Swee Tian is the Head and Senior Consultant of the Department of Diagnostic Imaging at the National University Hospital. Apart from being the Clinical Director of BreastScreen Singapore Programme of the National University Health System, he is also sitting on the Executive Committee of the National University Cancer Institute, Singapore (NCIS). A/Prof Quek graduated from the National University of Singapore (NUS) and embarked on his Radiology training, by obtaining the Fellowship of the Royal College of Radiologists in 1995. He underwent further training in musculoskeletal radiology at several centres in the UK. His areas of interest are in Musculoskeletal, Oncologic/Body and Breast Imaging. A/Prof Quek was previously a Senior Consultant in the Department of Oncologic Imaging, National Cancer Centre Singapore and held concurrent appointments as Visiting Consultant to the Department of Surgical Oncology at the National Cancer Centre, Department of Diagnostic Radiology at the Singapore General Hospital and the Ministry of Defence, Singapore. He is also a Council member of the College of Radiology of Singapore and sits on the College’s Steering Committee on Professional Standards and the Teleradiology Audit Committee in the Ministry of Health, Singapore. He has published on various topics in oncologic, musculoskeletal and breast imaging. Specialist in Focus A/Prof Quek Swee Tian Head and Senior Consultant, Department of Diagnostic Imaging 1 Could you share with us about the Department of Diagnostic Imaging’s role in shaping clinical care delivery in NUH? Imaging is an important aspect of the diagnostic process and has changed clinical care delivery in various ways. For example, the availability of a CT scanner in the Emergency Department has facilitated faster and more accurate assessment of the extent of injury in polytrauma patients, allowing for quicker and better surgical management. It is also commonly 18 • MED I CO J ULY - se ptemb er 2 014 used to assess patients with acute stroke for suitability for thrombolytic treatment, leading to a more personalised treatment with better outcome. Even in conditions like suspected appendicitis or pancreatitis, there is increasing reliance on imaging to confirm the diagnosis and look for possible complications to avoid unnecessary surgery and/or provide for a better pre-operative roadmap. In cancer treatment, imaging is crucial for staging the extent of disease and determining the optimal type of treatment (i.e. surgery, chemotherapy, or radiation therapy). As such, a review of the patient’s scans forms an important component in multidisciplinary tumour board discussions where patient management is deliberated. It is also used to assess treatment response and optimise treatment by switching to a different chemotherapeutic regime if there is poor response to firstline chemotherapy. Besides the diagnostic aspect, the therapeutic aspect of radiology has also changed clinical care delivery in some ways. Radiologists are able to offer patients and referring physicians a host of treatment options ranging from simple image-guided biopsies and drainages to more complex procedures like coiling or stenting of aneurysms. These treatment options are less invasive and may obviate the need for open surgery, resulting in shorter hospital stays and less severe/ fewer post-procedure complications. So, not surprisingly, we are seeing an increasing number of requests for such treatments in lieu of more conventional open surgery. 2 How will it support the primary healthcare/GPs in Singapore? Although we are a hospital-based practice, we have always been supportive of the primary healthcare sector. We provide reporting services for radiographs, ultrasound, and mammograms done at some polyclinics. GPs are also welcome to use our imaging services, be it simple screening chest X-rays, mammograms, or more complex examinations such as CT scan. In addition, we have also organised talks for GPs on various aspects of imaging such as screening CT colonoscopy and low dose CT for lung cancer screening to keep them updated on these topics. 3 How do you see the transformation of the Diagnostic study – in the past, present, and future? In the past, there was a lot of emphasis on the plain film (X-rays). While this is still important and will stay with us, going forward, there will be an increase in reliance and use of more complex cross-sectional imaging modalities like ultrasound, CT and MRI. These techniques require more detailed anatomical knowledge and more time to interpret as they may run into hundreds of images, particularly with reconstructed images or additional sequences performed. However, it is well worth the while as they provide us with important additional information Figure 1. Prof Quek and his children that can aid diagnosis and patient management. A good example is the imaging of head injuries. In the past, we usually obtain two or three different radiographs to assess patients with head injury. Nowadays, we would perform a CT for such patients. Although there are more images to review, it is a faster examination to perform and provides a much better assessment of the extent of head injury (e.g. intracranial haematoma, midline shift, skull fracture) if any. The information gained is much more comprehensive than with plain radiographs and thus results in better patient management. Some of the changes that have come about are due to changes in technology in other areas. For example, we are performing fewer Barium studies nowadays as improvements in fibre-optic technology have resulted in Bariums being partly replaced by gastroscopy and colonoscopy. There is certainly much more reliance on information technology. While the films in the past were physically cumbersome to transport and required large film archives to store, many institutions now have a digital picture archiving and communication system (PACS). This enables easy retrieval and review of images by both the radiologists and clinicians and has also allowed for teleradiology services. Crystal ball gazing is an imperfect art, but looking at the future, I believe the trend will be towards more hybrid and molecular imaging which may provide a more personalised patient diagnosis and treatment, and further development and use of interventional radiology services. 4 You have particular interests in Musculoskeletal, Oncologic/Breast Imaging. What inspired you to specialise in these areas? When I graduated in Radiology, MRI was in vogue then. So, it was a toss between Neuroradiology and Musculoskeletal (MSK) Imaging. I found MSK more stimulating as it involves multiple joints and body regions. We also had a very good working relationship with the Orthopaedics Department whom we met weekly to review interesting cases, so I decided on MSK with a slant towards MSK tumours and sports imaging. 2 014 JULY - S E P T E MB E R M EDICO • 19 Oncologic and breast imaging was something I stumbled into by accident rather than by design. I worked at the National Cancer Centre for some years and found oncologic and breast imaging challenging and interesting, in particular, the participation in the multidisciplinary tumour boards, where I could interact and work closely with colleagues in other disciplines, was intellectually stimulating and academically satisfying. And as a member of BreastScreen Singapore since its inception, it was great to see the growth and development of the programme. When we first started, some of the breast tumours were quite large at detection, but with time, we are now detecting more of the smaller and earlier stage tumours that carry a better prognosis. It is quite gratifying to know that the programme has done some good and that I have a chance to be part of it. 5 Could you share with us the more recent developments and breakthroughs in these areas that may result in better patient care? Advances in imaging have revolutionised many aspects of clinical practice in the last decade but I will only highlight a few. In breast imaging, the development of digital mammography is a significant step forward. It is easier and faster to perform and gives a higher level of detail than conventional film-screen technology. This means the patient spends less time in an uncomfortable position and is less likely to have to return for a repeat scan due to over or under-exposure. And being digital, it is easy for the images to be sent to a hospital for reading if the mammograms are done elsewhere, e.g., in the polyclinics, thus facilitating breast screening. There is also a newer technology known as breast tomosynthesis. This takes multiple X-ray images of the breast from different angles. The early results seem quite promising as the procedure is more comfortable and appears to enable us 20 • ME D ICO J ULY - se ptemb er 2 014 Figure 2. Prof Quek (fourth from left) during NUS Commencement 2014 to detect breast cancers more easily in women with dense breasts. With CT, many of the recent technological advances have resulted in dose reduction, reduction in scan time, as well as scan results with greater detail (thinner slices). CT also provides better depiction of both the anatomy and pathology, allowing for more accurate diagnosis. A good example is CT angiography. In the past, patients with suspected pulmonary embolism were investigated with a lung ventilation/ perfusion (V/Q) scan which took about 30 minutes to an hour to perform, and was difficult to be interpreted, particularly in sick patients who could not ventilate well. Nowadays, this can be easily assessed with a contrast CT which takes only a few minutes to perform and gives exquisite images that are easier and more accurate to read. Likewise, patients with suspected clot or aneurysm causing a stroke can be assessed first with a CT angiogram instead of a conventional catheter angiogram (which takes longer to organise and perform and is a more invasive procedure that carries a higher risk of complications). CT angiography can also be performed for non-invasive assessment of the coronary arteries. Improvement in MR technology has also allowed for some of these angiographic procedures to be performed by MRI. The widespread use and acceptance of MRI in clinical practice is a reflection of its place in providing for better patient care ranging from early detection of stroke to accurate assessment of internal derangements of joints (without having to resort to more invasive arthroscopy) and pre-surgical assessment of the extent of disease (e.g. rectal, cervical, and prostate cancer) to guide management for a better outcome. In nuclear medicine, a major technological breakthrough was the integration of PET (Positron Emission Tomography) with CT, a process in which one of my colleagues, David Townsend, played a key role. The place of PET-CT in the staging of certain tumours is now firmly established and it has helped to optimise treatment for these cancers and obviate unnecessary surgery. I have also mentioned earlier that the advances in Interventional Radiology allow us to treat patients with a wide variety of disorders using techniques that are less invasive than open surgery, so that patients will have a faster recovery period and fewer associated complications. 6 What other responsibilities do you have? I am quite involved in the national breast screening programme and sit in a few of the committees there, namely the Advisory, the Quality Assurance & Training as well as the Audit Committees. The roles include planning the direction of the BreastScreen Singapore (BSS) programme as well as auditing the programme to ensure a high level of quality assurance. I also chair a committee organising the Breast Screen Singapore Seminar in October this year which will coincide with the Breast Cancer Awareness Month. As an extension of my interest in oncologic work, I am an EXCO member of the National University Cancer Institute, Singapore (NCIS) and a member of the Working Committee of the Western Cancer Action Network (WCAN). On the NUH front, I am part of a group of Senior Advisors to the NUHS Medico-Legal Team and also sit in the Singapore Medical Council Complaints and Disciplinary Committee. Some of my other responsibilities include Figure 3. Prof Quek with colleagues at NUHS Tower Block being an Editorial Board member for the Journal of Radiology and helping to plan for Radiology training in Singapore as a member of the Specialist Training Committee for Diagnostic Radiology in the Ministry of Health. 7 What areas do you hope to focus on in your future career? Any particular reasons? I hope to be able to spend more time in the field of Medical Education and Training. Medicine has traditionally been taught by apprenticeship, but it is good to make it a more structured process. IT has also changed the way things are taught, in particular in Radiology. For example, our trainees are given practice sets to do online at their own convenience and we then meet to discuss the findings. Training and education are important as they help us to maintain and improve on our professional competency and ensure that we produce better doctors with each succeeding generation. Of course, as one of my colleagues pointed out, the selfish side to it is that we will all grow old and be looked after by the current younger generation of doctors one day, so it pays for us to train them well now! 8 Where do you see yourself in the next 5 years in terms of career, personal, social and family life? I hope to have built a good team of younger radiologists who can take over the running of the Department and carry it to greater heights. That will leave me more time to spend with my family and for myself. 2 014 JULY - S E P T E MB E R M EDICO • 21 M EDIC AL N O TES A/Prof Thomas Choudary Putti Senior Consultant and Clinical Director, Department of Pathology Associate Professor Thomas Choudary Putti graduated from the Osmania University, Hyderabad, India in 1985 with MBBS. His initial training in Histopathology was at the Department of Pathology, Osmania Medical College and he obtained his specialist degree in pathology from the Osmania University, India in 1989. Subsequently, he did his anatomic pathology residency from Long Island Jewish Medical Centre, New York and obtained his American Board Certification in 1997. He did a year of fellowship in Immunopathology from Bronx-Lebanon Hospital, New York from 1997 - 1998. He had a six-month stint as clinical fellow (breast pathology) at Nottingham City Hospital, UK under the guidance of Prof. Ian Ellis. He is currently a Senior Consultant and Clinical Director in the Department of Pathology at NUH and has been with the department for the last 15 years. He is also an affiliated member and Senior Consultant with the National University Cancer Institute, Singapore (NCIS). Pathology and NCIS The Department of Pathology at the National University Hospital (NUH) provides a comprehensive range of diagnostic services using innovative technology and highly-trained personnel. It services the diagnostic requests of numerous medical specialties and plays a critical role in the process of patient diagnosis, treatment, and monitoring. The department performs in excess of 40,000 histopathology and cytology tests per year. Our specialist surgical pathologists play a definitive role in tumour diagnosis. Despite a high index of clinical suspicion and radiological support, the diagnosis of cancer is not conclusively established in the absence of tissue diagnosis. Surgical pathologists provide an accurate and sufficiently comprehensive diagnosis that enables the clinician to develop an optimal treatment plan and provide prognostic indicators. Figure 1. Diagnostic Molecular Oncology Centre team 22 • ME D ICO J ULY - se ptemb er 2 014 The tremendous advances in all fields of oncology require a great deal of additional information to allow the most appropriate classification for research, prognosis and therapeutic intervention. Our pathologists actively contribute to several multi-disciplinary tumour boards. A comprehensive range of diagnostic services provided by our department include: • Routine and specialised surgical pathology work • Intra-operative/frozen section consultation • Expert consultation for subspecialty • Gynaecological and nongynaecological cytology Figure 2. Interpretation of Fluorescence in-situ hybridisation by Molecular pathologist and technologist The Diagnostic Molecular Oncology Centre (DMOC) is a laboratory section of the NUH Department of Pathology, which is accredited by the College of American Pathologists (CAP). DMOC focuses on the molecular diagnosis of solid tumours involving the integrated molecular analysis of routine clinical samples reported by surgical pathologists and cytopathologists. Diagnostic Molecular Oncology Centre The Diagnostic Molecular Oncology Centre (DMOC) is a laboratory section of the NUH Department of Pathology, which is accredited by the College of American Pathologists (CAP). DMOC focuses on the molecular diagnosis of solid tumours involving the integrated molecular analysis of routine clinical samples reported by surgical pathologists and cytopathologists. This collaborative paradigm is at the core of stratified oncology or therapeutic pathology. The laboratory specialises in tissuebased molecular diagnosis and, in particular, in the interfacing among tissue morphology, immunohistochemistry, in-situ hybridisation (ISH) techniques, polymerase chain reaction (PCR) based sequencing, and fragment analysis technology, providing a one stop laboratory for integrated pathology tissue diagnosis. Figure 3. FNA clinic; FNA procedure (above) and Interpretation of FNA smears by cytology team (below) DMOC is currently a reference laboratory for the development of high-quality molecular testing in the area of personalised/stratified oncology, and is also involved in sample logistics for several on-going clinical trials in the National University Cancer Institute, Singapore (NCIS) involving next generation sequencing (NGS) analysis of archival clinical materials for the panelled oncogene profiling of solid tumours for drug-able targets, in a collaborative partnership with the Centre for Translational Research and Diagnostics (CTRAD) and clinician scientists from the NCIS. Fine needle aspiration (FNA) service FNA is a quick, minimally invasive test to obtain diagnostic material from a tumour or lump. It is an effective rapid test in determining adequacy of the sample and providing immediate preliminary results. It is also extremely useful in the diagnosis and treatment of cysts. Fine needle aspiration is a type of biopsy in which cells are removed from a lump either with only a needle or with a needle and syringe. The cells are evaluated under a microscope to determine the nature of the lump. Special tests can be applied to these small samples to aid in the diagnosis and treatment of cancer, including tumours of the breast, lymph nodes and thyroid. An immediate provisional diagnosis is provided followed by a final report within two days of the procedure. At the NUH Medical Centre FNA Clinic (Level 15), specialised pathologists called cytopathologists who diagnose diseases at the cellular level offer consultation services. They perform the procedure and provide immediate provisional diagnosis, thereby allowing the clinicians to plan management of the disease in the same visit. 2 014 JULY - S E P T E MB E R M EDICO • 23 UPCOMING EVENTS NUH GP CME Programme 2014 Please refer to our GPLC website for online registration. September SATURDAY October 20 National University Heart Centre, Singapore NUHCS Cardiology Updates Living and Managing Heart Disease: Adult Congenital and Structural Heart Disease SATURDAY 18 University Medicine Cluster NUH Gastroenterology Updates Event information listed is correct at time of print. While every attempt will be made to ensure that all events will take place as scheduled, the organisers reserve the rights to make appropriate changes should the need arises. Please refer to our events calendar at www.nuh.com.sg/nuh_gplc for more updates and information. A Publication of NUH GP Liaison Centre (GPLC) Advisor A/Prof Goh Lee Gan Editors Jaime Raniwaty Chiah and Davin Wangsa Editorial Member Lisa Ang We will love to hear your feedback on Médico. Please direct all feedback to: The Editor, Médico GP Liaison Centre, National University Hospital 1E Kent Ridge Road, NUHS Tower Block, Level 6, Singapore 119228 Tel: 6772 5079 Fax: 6777 8065 Email: [email protected] Website: www.nuh.com.sg/nuh_gplc Co. Reg. No. 198500843R The information in this publication is meant purely for educational purposes and may not be used as a substitute for medical diagnosis or treatment. You should seek the advice of your doctor or a qualified healthcare provider before starting any treatment, or, if you have any questions related to your health, physical fitness or medical condition(s). Copyright (2014). National University Hospital, Singapore All rights reserved. No part of this publication may be reproduced without permission in writing from National University Hospital. The NUHS group
© Copyright 2026 ExpyDoc