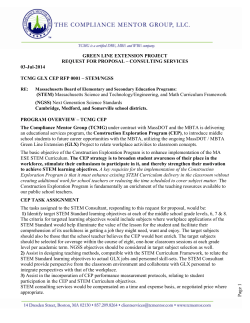
The Journal of Arthroplasty xxx (2014) xxx–xxx Contents lists available at ScienceDirect The Journal of Arthroplasty journal homepage: www.arthroplastyjournal.org A 5–8 Year Retrospective Follow-Up of the C-Stem AMT Femoral Component: Patient Reported Outcomes and Survivorship Analysis James R. Berstock, MBChB, MRCS , Michael R. Whitehouse, PhD, MSc (Orth Eng), FRCS (Tr&Orth), Danielle C. Piper, Stephen J. Eastaugh-Waring, MB, ChB, FRCS (Tr&Orth), Ashley W. Blom, MD, PhD, FRCS (Tr&Orth) University of Bristol Musculoskeletal Research Unit, AOC (Lower Level), Southmead Hospital, Westbury-on-Trym, Bristol, UK a r t i c l e i n f o Article history: Received 17 February 2014 Accepted 27 April 2014 Available online xxxx Keywords: hip arthroplasty replacement bone cement treatment outcome survival rate a b s t r a c t We report midterm functional, radiographic and survivorship data for the cemented, triple taper C-stem AMT femoral component from a consecutive cohort of 415 hip arthroplasties in 386 patients at a non-developer centre. Follow-up ranges were from 60 to 99 months, with a mean of 76 months. 32 hips were lost to follow-up. The median OHS was 40, median SF-12 mental component score (MCS) was 50, and median SF-12 physical component score (PCS) was 39. At 99 months follow up, stem survivorship is 96.9% (95% confidence interval (CI) 82.5–99.5), and construct survivorship is 96.0% (95% CI 84.2–99.0). Adverse events such as calcar fracture, greater trochanter fracture and dislocation were rare at b 1%. There have been no revisions for aseptic loosening. © 2014 Elsevier Inc. All rights reserved. The prevalence of osteoarthritis continues to increase and it will represent the fourth leading cause of disability worldwide by 2020 [1]. The demand for total hip arthroplasty (THA) is predicted to rise by 174% between 2003 and 2030 [2]. In England and Wales, approximately equal numbers of cemented and cementless implants are used. Registry data from the National Joint Registry for England, Wales and Northern Ireland indicate higher early to midterm survivorship of cemented implants compared to cementless implants [3]. For the most often used combinations in each category, the cumulative percentage probability of first revision at 5 and 8 years were 1.39% (95% CI 1.26–1.52) and 2.11% (95% CI 1.88–2.37) for cemented implants (Exeter/Contemporary; Stryker, Newbury, UK) and 3.14% (95% CI 2.94–3.34) and 5.89% (95% CI 5.11–6.79) respectively for cementless implants (Corail/Pinnacle; DePuy Int., Leeds, UK). There are potential confounding factors in survivorship analysis such as age, activity, bearing size and bearing couple. Aseptic loosening is the most common cause of failure in THA [1,4]. The taper slip cemented stem design has proven successful in nondeveloper centres [5,6] and it has been suggested that the original polished, flat-back Charnley femoral component may have acted as a taper slip [7]. Bone resorption secondary to stress shielding leads to a reduced survival of prostheses [8], particularly in the case of calcar bone loss [9]. Calcar bone loss may lead to more complex revision surgery being required. Periprosthetic bone mineral density (BMD) has been consistently shown to decrease following cemented THA [10,11] with the greatest loss (up to 20% of bone stock) in Gruen zone 7 [12]. Double taper designs such as the Exeter stem and the CPT stem (Zimmer Ltd., Swindon, UK) taper in the craniocaudal and the anteroposterior directions. In the triple taper design, a third taper is added from lateral to medial with the intention of loading the proximal femur, particularly the calcar to reduce resorption [13]. Despite this, reduction in BMD is still seen in triple taper designs but with improved preservation of medial compared to lateral zones [14]. Comparison of a triple taper (C stem; DePuy Int., Leeds, UK) and a double taper design (Exeter Universal) has shown no differences in clinical scores, complications or subsidence [15]. The original C stem design (DePuy Int., Leeds, UK) was modified to permit a more controlled insertion by the addition of a shoulder to the stem, the addition of a high offset option and a change in the taper to a 12/14 geometry (mini Articul/EZE) to create the C stem AMT, which is the subject of this report. The aim of this study was to ascertain the functional, radiological and survivorship outcomes of the triple tapered cemented stem in a multisurgeon, single centre study at a minimum follow up of five years. Materials and Methods The Conflict of Interest statement associated with this article can be found at http:// dx.doi.org/10.1016/j.arth.2014.04.034. Reprint requests: James R. Berstock, MBChB, MRCS, University of Bristol Musculoskeletal Research Unit, AOC (Lower Level), Southmead Hospital, Westbury-on-Trym, Bristol, BS10 5NB, UK. Between March 2005 and April 2008, a consecutive series of 415 primary C-stem AMT hip arthroplasties in 386 patients were performed under the care of three surgeons at our institution. The http://dx.doi.org/10.1016/j.arth.2014.04.034 0883-5403/© 2014 Elsevier Inc. All rights reserved. Please cite this article as: Berstock JR, et al, A 5–8 Year Retrospective Follow-Up of the C-Stem AMT Femoral Component: Patient Reported Outcomes and Survivorship Analysis, J Arthroplasty (2014), http://dx.doi.org/10.1016/j.arth.2014.04.034 2 J.R. Berstock et al. / The Journal of Arthroplasty xxx (2014) xxx–xxx C-stem AMT was implanted with an Ogee cup (DePuy Int., Leeds, UK) in 52% of cases, and a Pinnacle cup (DePuy Int., Leeds, UK) in 44%. When all the patients had reached the 5-year anniversary of surgery (range 60–99 months), functional questionnaires were sent out by mail. We used the Oxford hip score [16] (OHS), Short Form-12 Health Survey [17] (SF-12), and the Self-Administered Patient Satisfaction Scale [18]. In the event of non-response, reminders were sent by post before the patients were contacted by telephone. We also asked directly about subsequent hip surgery to identify those who may have had revision surgery in other units. Non-responders were contacted by telephone to complete questionnaires. Where medical problems prevented completion of questionnaires, collateral history was taken from carers to ensure no revision surgery had occurred. The quality of the cement mantle on the immediate postoperative radiograph was assessed by the method described by Barrack et al [19]. The most recent follow-up radiograph was assessed for evidence of implant loosening in the zones described by Gruen et al [12], for evidence of progressive lucency, calcar resorption according to Engh [20], and osteolysis. The flow of patients through this study is provided in Fig. 1. Statistics Statistical analysis was performed using SPSS version 19 software (IBM Corporation, New York, USA). The distribution of data was tested using the Kolmogrov–Smirnov statistic. Normally distributed data are reported as a mean and standard deviation and tested with a two-tailed t-test, whereas non-parametric data are reported as a median and interquartile range, and tested with the independent samples Kruskal–Wallis test. Implant survivorship was analysed using Kaplan–Meier survivorship curves with 95% confidence intervals. Patients with surviving implants were censored at either the time of most recent questionnaire, radiograph, or upon death. Results Surgical Characteristics The mean age of the patients at time of surgery was 74 years (range 39–92), with a 66% female preponderance. The indication for surgery was osteoarthritis in 97% of cases, with 57% of cases performed through a posterior approach and an omega approach used for the remainder. Metal on polyethylene bearings were used in 84%, metal on metal in 9%, ceramic on ceramic in 7%, and ceramic on polyethylene in b 1%. Intraoperatively there were two calcar cracks (0.5%) both treated with cables, and two greater trochanter fractures (0.5%), both reattached with tension band wires. Follow-Up As summarised in Fig. 1, 86 patients with 93 hips (22%) had died at the time of final follow-up. Medical problems prevented 17 patients (4%) from completing forms. Seven patients (2%) declined participation. In total, of the 298 hip eligible for ongoing inclusion, 266 questionnaires were returned, OHSs for 2 of these were only partially complete, with 32 (11%) hips lost to follow-up. The mean questionnaire follow-up period was 76 months, (range 60– 99 months). Recent pelvic radiographs were available for all 32 patients lost to questionnaire follow-up at a mean of 30 months (range 3–73). There was no statistically significant difference in age at surgery between the group lost to follow-up and the remaining patients (two-tailed t-test P = 0.17). Fig. 1. Flow diagram of study follow up. Please cite this article as: Berstock JR, et al, A 5–8 Year Retrospective Follow-Up of the C-Stem AMT Femoral Component: Patient Reported Outcomes and Survivorship Analysis, J Arthroplasty (2014), http://dx.doi.org/10.1016/j.arth.2014.04.034 J.R. Berstock et al. / The Journal of Arthroplasty xxx (2014) xxx–xxx 3 Radiographic follow-up occurred in 401 patients (97%) at a mean of 40 months post-operatively. Follow-up reporting is summarised in Table 1. Survivorship There have been two stem revisions and four acetabular revisions. Single component C-stem AMT Kaplan–Meier survivorship at 99 months is 96.9% (95% CI 82.5–99.5), see Fig. 2. Construct survivorship is 96.0% (95% CI 84.2–99.0). The two stem revisions were both for sepsis, occurring at 24 and 88 months post-operatively. Both patients underwent successful two-stage revision of both components. Two other patients underwent single component acetabular revisions, one to a constrained liner at 38 months following recurrent dislocations, and one for presumed aseptic loosening at 88 months. In the case of acetabular loosening, tissue specimens sent as a precaution at the time of revision were positive for microorganisms and a course of antibiotics was commenced. The stem was not revised, and the patient has been clinically free of infection without antibiotics for 18 months. A total of four patients (1%) experienced one or more dislocations. There was one immediate postoperative dislocation, one late dislocation, and one patient experienced two late dislocations. All were treated by closed reduction, and have not required revision, except the case revised to a constrained liner discussed above. Two other patients have had soft tissue hip procedures, one for trochanteric bursitis and one for abductor muscle reattachment. There has been one postoperative greater trochanter fracture, and one Vancouver C periprosthetic fracture, both treated with open reduction and internal fixation without stem revision. Clinical results At a minimum five-year follow-up, the median OHS was 40 (on a scale of 0–48 with 48 representing best function [21]), with an interquartile range (IQR) of 15. Postoperative OHSs are summarised in Fig. 3. The median SF-12 MCS score was 50 (IQR 20) and PCS score was 39 (IQR 22). Median satisfaction score was 100 (IQR 19). There was no significant difference in functional outcome between the different bearing types, independent samples Kruskal–Wallis test P = 0.41. Radiographic results Fig. 2. Single component C-stem AMT Kaplan–Meier survivorship curve. was available for 401 (97%) of patients. Of these, 61% had some radiographic lucency in one or more Gruen zones. The commonest zones of lucency were zone 1 (55% of stems) and zone 7 (in 35% of stems implanted). No polymethylmethacrylate fractures were identified. One osteolytic lesion has been noted and there are three cases of progressive lucency, none of which has been revised. Calcar resorption was evident in 5% of cases, as per Engh grading [18] which is summarised in Table 2. Discussion Cemented total hip arthroplasty is one of the most cost effective and successful surgical interventions available today. In our retrospective cohort, the C-stem AMT femoral component showed excellent survivorship of 96.9% (95% CI 82.5–99.5), and construct survivorship is 96.0% (95% CI 84.2–99.0) at 99 months follow-up. These results are similar to previous survivorship reports of the original C-stem femoral component [13]. The only other study of the C-stem AMT that we are aware of reports encouraging results with no loosening, subsidence, dislocation or revision at a mean 9 month follow-up in a cohort of 34 patients [22]. Implant survivorship in this series compares favourably with data from the National Joint Registry for England, Wales and Northern Ireland [3], despite 9% of the constructs having metal-on-metal bearing surfaces. Metal-on-metal Of the 415 hips, immediate post-operative radiographs were available for 398 (96%). The majority of those were not available predate the upgrade to the computerised Picture Archiving Communication Service (PACS). Cementation was graded on immediate postoperative radiographs as Barrack A in 60%, B in 38%, and C in 2%. A follow-up radiograph taken at a mean of 39 months post-operatively Table 1 Summary of Follow-Up Details. Original Number of Patients in Study Number of Hips at Start of Study Number of Hips Lost Due to Patients Death Number of Hips Lost to Follow-Up Number of Hips Revised for Any Reason Number of Hips Surviving at End of Study Number of Patients Examined Number of Patients Questionnaire/Telephone Review Mean Follow-Up and Range Revisions Follow-Up Period Kaplan–Meier Survival 386 415 93 32 4 (2 both component revisions and 2 single component acetabular revisions) 294 0 266 76 months (60–99) 4 99 months 96.0% (95% CI 84.2–99.0) Fig. 3. Chart of postoperative Oxford hip scores. Please cite this article as: Berstock JR, et al, A 5–8 Year Retrospective Follow-Up of the C-Stem AMT Femoral Component: Patient Reported Outcomes and Survivorship Analysis, J Arthroplasty (2014), http://dx.doi.org/10.1016/j.arth.2014.04.034 4 J.R. Berstock et al. / The Journal of Arthroplasty xxx (2014) xxx–xxx Table 2 Engh Grading of Calcar Resorption. Grade 0 Grade 1 Grade 2 Grade 3 Grade 4 381 (95%) 9 (2%) 10 (2%) 1 (b1%) 0 (0%) bearings have been shown to have high failure rates [23] and thus it is somewhat fortuitous that none of the metal-on-metal bearings in this series has required revision to date. The median OHS for the 39 patients with metal-on-metal bearings was 39, representing slightly worse scores than the median for the whole cohort. This difference was not statistically significant. Although our data also compare favourably with that of cementless stems reported in the National Joint Registry for England Wales and Northern Ireland, we point out the older age at surgery in our cohort, and that in our unit, this stem was preferentially utilised in older patients which may impact the survivorship in patients not in that demographic set with longer follow up. Compared with the original C-stem, which has now achieved a 10A Orthopaedic Device Evaluation Panel (ODEP) rating within the UK, the C-stem AMT has undergone design changes meaning that the C-stem AMT is a new entity according to ODEP, and is currently 7B rated. This means that currently, only weak data exist to support a failure rate of less than 7% at 7 years. To achieve the top 10A rating, strong evidence of a failure rate of less than 10% at 10 years follow-up must exist. Like many other collarless polished cemented stems, the C-stem draws on the taper-slip philosophy, which depends on controlled subsidence of the tapered stem due to natural cement creep [24,25]. The importance of this slip philosophy was demonstrated by the relative failure of a matte coated Exeter stem [26]. Double taper implants e.g. CPT and Exeter are tapered in the anteroposterior plane and mediolateral planes. These stems have excellent results out to 10 years at independent centres [6,27]. Occasionally, excessive subsidence has been associated with cement mantle fracture, and failure of the femoral component in these double taper devices [6,28,29]. The C-stem was the first taper-slip stem to employ a triple taper design, however some previous matte finished stems were also triple tapered. This additional third taper is from the wide lateral to the narrow medial plane, making the stem slightly oval in cross-section. Clinical evidence in support of the triple taper design in the form of positive bone remodelling at the medial calcar has been observed radiographically after C-stem implantation [13,30,14], however the most recent randomised trial has not shown a significant clinical difference between double taper and triple taper designs [31]. A further clinical trial has been set up to compare radiostereometric subsidence following C-stem AMT and Exeter stem implantation (trial identifier: NCT00722982). In this study, we observed good proximal bone preservation, with 95% of cases showing no calcar resorption (Engh grade 0) [20]. This is an improvement on the results reported by Hook et al [6], suggesting only 26% grade 0 calcar resorption with the Exeter stem at 10 year minimum follow-up. However, our radiographic follow-up occurred at a mean of only 39 months, so we may observe additional calcar resorption with longer follow-up. The rate of periprosthetic joint infection in our series was 3 out of 415 cases (0.7%) which is at the lower end of the range reported by other authors [32–35]. There have been no revisions for aseptic loosening at this stage, representing a potential cost saving if these results are maintained. In line with good research practise in arthroplasty cohort studies, we report both clinical and survivorship outcomes [36]. The median postoperative OHS of 40, is similar to that found in other series of comparable length follow-up [37,38]. This equates to a good outcome using the Harris hip score [38]. The ceiling effect of the OHS is evident in Fig. 3, affecting 9% of patients which is acceptable, but reflects the score’s inability to differentiate between the best performing patients. Our study is limited by a lack of pre-operative scores and losses to follow-up. Every effort was made to contact the 32 patients lost to follow-up. We presume that these patients had either died or moved to other regions, as we were unable to make contact. All the patients lost to follow-up had undergone radiographic assessment during the five years following surgery, with no evidence of failure or revision, and for the purpose of Kaplan–Meier survivorship these patients are censored at the time of radiographic assessment. The fate of all other implants is known, including in the deceased. Our rate of loss to follow-up is comparable with other similar sized cohorts beyond five years [39–42]. The C-stem AMT demonstrates excellent implant survivorship at 5–8 year follow-up, as well as good midterm functional outcome. Aseptic femoral component loosening has yet to be observed at midterm review of this consecutive series of C-stem AMT hip arthroplasties. Despite continued improvements in implant design and cementing techniques, aseptic loosening remains the leading cause of late failure and revision of cemented femoral stems [3,25,43,44]. Hence there is a need for longer term surveillance of this series. References 1. Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ 2003;81–9:646. 2. Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 2007;89A–4:780. 3. National Joint Registry for England, Wales and Northern Ireland 10th Annual Report 2013. Available at http://www.njrcentre.org.uk/njrcentre/Portals/ 0/Documents/England/Reports/10th_annual_report/NJR%2010th%20Annual% 20Report%202013%20B.pdf . [date last accessed 1 April 2014]. 4. Malchau H, Herberts P, Ahnfelt L. Prognosis of total hip-replacement in Sweden follow-up of 92,675 operations performed 1978–1990. Acta Orthop Scand 1993;64–5:497. 5. Burston BJ, Barnett AJ, Amirfeyz R, et al. Clinical and radiological results of the collarless polished tapered stem at 15 years follow-up. J Bone Joint Surg (Br) 2012;94B–7:889. 6. Hook S, Moulder E, Yates PJ, et al. The Exeter Universal stem: a minimum ten-year review from an independent centre. J Bone Joint Surg (Br) 2006;88B–12:1584. 7. Shen G. Femoral stem fixation. An engineering interpretation of the long-term outcome of Charnley and Exeter stems. J Bone Joint Surg (Br) 1998;80B–5:754. 8. Kobayashi S, Saito N, Horiuchi H, et al. Poor bone quality or hip structure as risk factors affecting survival of total-hip arthroplasty. Lancet 2000;355–9214:1499. 9. Carlsson AS, Gentz CF. Mechanical loosening of the femoral-head prosthesis in the Charnley total hip-arthroplasty. Clin Orthop Relat Res 1980;147:262. 10. Damborg F, Nissen N, Jorgensen HRI, et al. Changes in bone mineral density (BMD) around the cemented Exeter stem - a prospective study in 18 women with 5 years follow-up. Acta Orthop 2008;79–4:494. 11. Kroger H, Miettinen H, Arnala I, et al. Evaluation of periprosthetic bone using dualenergy X-ray absorptiometry: precision of the method and effect of operation on bone mineral density. J Bone Miner Res 1996;11–10:1526. 12. Gruen TA, McNeice GM, Amstutz HC. "Modes of failure" of cemented stem-type femoral components: a radiographic analysis of loosening. Clin Orthop Relat Res 1979;141:17. 13. Wroblewski BM, Siney PD, Fleming PA. Triple taper polished cemented stem in total hip arthroplasty: rationale for the design, surgical technique, and 7 years of clinical experience. J Arthroplasty 2001;16–8(Suppl. 1):37. 14. Buckland AJ, Dowsey MM, Stoney JD, et al. Periprosthetic bone remodeling using a triple-taper polished cemented stem in total hip arthroplasty. J Arthroplasty 2010;25–7:1083. 15. Ek ET, Choong PF. Comparison between triple-tapered and double-tapered cemented femoral stems in total hip arthroplasty: a prospective study comparing the C-Stem versus the Exeter Universal early results after 5 years of clinical experience. J Arthroplasty 2005;20–1:94. 16. Dawson J, Fitzpatrick R, Carr A, et al. Questionnaire on the perceptions of patients about total hip replacement. J Bone Joint Surg (Br) 1996;78B–2:185. 17. Ware JE, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996;34–3:220. 18. Mahomed N, Gandhi R, Daltroy L, et al. The self-administered patient satisfaction scale for primary hip and knee arthroplasty. Arthritis 2011;2011:591253. 19. Barrack RL, Mulroy Jr RD, Harris WH. Improved cementing techniques and femoral component loosening in young patients with hip arthroplasty. A 12-year radiographic review. J Bone Joint Surg (Br) 1992;74(B-3):385. 20. Engh CA, Bobyn JD, Glassman AH. Porous-coated hip-replacement - the factors governing bone ingrowth, stress shielding, and clinical-results. J Bone Joint Surg (Br) 1987;69B–1:45. Please cite this article as: Berstock JR, et al, A 5–8 Year Retrospective Follow-Up of the C-Stem AMT Femoral Component: Patient Reported Outcomes and Survivorship Analysis, J Arthroplasty (2014), http://dx.doi.org/10.1016/j.arth.2014.04.034 J.R. Berstock et al. / The Journal of Arthroplasty xxx (2014) xxx–xxx 21. Murray DW, Fitzpatrick R, Rogers K, et al. The use of the Oxford hip and knee scores. J Bone Joint Surg (Br) 2007;89B–8:1010. 22. Spitzer A, Waltuch I, Goodmanson P, et al. Triple tapered polished collarless cemented stem: early experience with an enhanced extramedullary design. J Bone Joint Surg (Br) 2008;90B(Suppl. III):508. 23. Smith AJ, Dieppe P, Vernon K, et al. Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales. Lancet 2012;379–9822:1199. 24. Shah N, Porter M. Evolution of cemented stems. Orthopedics 2005;28(8 Suppl.): s819. 25. Fowler JL, Gie GA, Lee AJ, et al. Experience with the Exeter total hip replacement since 1970. Orthop Clin North Am 1988;19–3:477. 26. Middleton RG, Howie DW, Costi K, et al. Effects of design changes on cemented tapered femoral stem fixation. Clin Orthop Relat Res 1998:355. 27. Yates PJ, Burston BJ, Whitley E, et al. Collarless polished tapered stem: clinical and radiological results at a minimum of ten years' follow-up. J Bone Joint Surg (Br) 2008;90B–1:16. 28. Rhyu KH, Lee SM, Chun YS, et al. Does osteoporosis increase early subsidence of cementless double-tapered femoral stem in hip arthroplasty? J Arthroplasty 2012;27–7:1305. 29. Dairaku K, Ishii M, Kobayashi S, et al. Initial evaluation on subsidence of cemented collarless polished tapered stem applied to the patients with narrow femoral medullar canal. Open Orthop J 2010;4:147. 30. sochart DH, Chaudhary N. Results of the C-Stem polished triple tapered femoral component. J Bone Joint Surg (Br) 2009;91B(Suppl. I):91. 31. Jayasuriya RL, Buckley SC, Hamer AJ, et al. Effect of sliding-taper compared with composite-beam cemented femoral prosthesis loading regime on proximal femoral bone remodeling: a randomized clinical trial. J Bone Joint Surg Am 2013;95A–1:19. 32. Webb BG, Lichtman DM, Wagner RA. Risk factors in total joint arthroplasty: comparison of infection rates in patients with different socioeconomic backgrounds. Orthopedics 2008;31–5:445. 5 33. Dowsey MM, Choong PFM. Obesity is a major risk factor for prosthetic infection after primary hip arthroplasty. Clin Orthop Relat Res 2008;466–1:153. 34. Pulido L, Ghanem E, Joshi A, et al. Periprosthetic joint infection: the incidence, timing, and predisposing factors. Clin Orthop Relat Res 2008;466–7:1710. 35. Bozic KJ, Ong K, Lau E, et al. Estimating risk in Medicare patients with THA: an electronic risk calculator for periprosthetic joint infection and mortality. Clin Orthop Relat Res 2013;471–2:574. 36. Wylde V, Blom AW. The failure of survivorship. J Bone Joint Surg Br 2011;93B– 5:569. 37. Wylde V, Blom AW, Whitehouse SL, et al. Patient-reported outcomes after total hip and knee arthroplasty comparison of midterm results. J Arthroplasty 2009;24– 2:210. 38. Kalairajah Y, Azurza K, Hulme C, et al. Health outcome measures in the evaluation of total hip arthroplasties - a comparison between the Harris hip score and the Oxford hip score. J Arthroplasty 2005;20–8:1037. 39. Garcia-Cimbrelo E, Garcia-Rey E, Cruz-Pardos A, et al. Stress-shielding of the proximal femur using an extensively porous-coated femoral component without allograft in revision surgery: a 5- to 17-year follow-up study. J Bone Joint Surg (Br) 2010;92B–10:1363. 40. Akiyama H, Yamamoto K, Tsukanaka M, et al. Revision total hip arthroplasty using a Kerboull-type acetabular reinforcement device with bone allograft: minimum 4.5year follow-up results and mechanical analysis. J Bone Joint Surg (Br) 2011;93B– 9:1194. 41. Mori T, Kudo H, Iwano K, et al. Kudo type-5 total elbow arthroplasty in mutilating rheumatoid arthritis - a 5-to 11-year follow-up. J Bone Joint Surg (Br) 2006;88B–7:920. 42. Sabouret P, Lavoie F, Cloutier JM. Total knee replacement with retention of both cruciate ligaments: a 22-year follow-up study. Bone Joint J 2013;95B–7:917. 43. Amstutz HC, Lodwig M. Wear of polymeric bearing materials: the effects of in vivo implantation. J Biomed Mater Res 1976;10–1:25. 44. Stauffer RN. Ten-year follow-up study of total hip replacement. J Bone Joint Surg Am 1982;64A–7:983. Please cite this article as: Berstock JR, et al, A 5–8 Year Retrospective Follow-Up of the C-Stem AMT Femoral Component: Patient Reported Outcomes and Survivorship Analysis, J Arthroplasty (2014), http://dx.doi.org/10.1016/j.arth.2014.04.034
© Copyright 2026 ExpyDoc