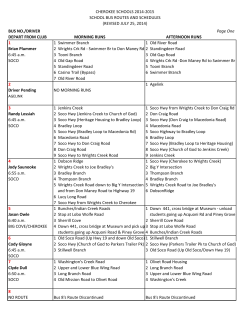
SOE1_SOE1.qxd 19-04-2013 19:25 Page 1 Structured oral examination 1 1 Long case 1 History A 70-year-old male patient underwent elective abdominal aortic aneurysm repair 24 hours ago. His past medical history includes hypertension and ischaemic heart disease. His medications up to the day of surgery included simvastatin 30mg o.d., enalapril 10mg o.d., atenolol 50mg o.d. and aspirin 75mg o.d. He smoked 20-30 cigarettes until 6 months ago, after which he completely stopped. The intra-operative blood loss was 1.2 litres with an aortic cross-clamp time of 65 minutes. The average urine output during the intra-operative period was 90ml/hour. Following the release of the aortic clamp, he required inotropic support for a brief period. He was transferred to the intensive care unit and ventilated overnight. Postoperative pain relief is still provided with epidural infusion of 0.125% bupivacaine and fentanyl 2mg/ml. He was weaned off the ventilator and extubated 4 hours ago. You have been called to see the patient as he has developed shortness of breath. Clinical examination He is conscious, breathless, sweaty and clammy. His peripheral oxygen saturation is 94% whilst breathing spontaneously 60% oxygen. On examining the chest there is bilateral equal air entry with crackles at both bases. Clinical Anaesthesia Information for the candidate SOE1_SOE1.qxd 19-04-2013 19:25 Page 2 2 The Structured Oral Examination in Clinical Anaesthesia Practice examination papers Table 1.1 Clinical examination. Weight Height Heart rate Blood pressure Temperature 78kg 170cm 120 bpm 95/65mmHg 36.9°C Investigations Table 1.2 Biochemistry. Sodium Potassium Urea Creatinine Blood glucose 138mmol/L 3.2mmol/L 14.5mmol/L 123mmol/L 8.5mmol/L Normal values 135-145mmol/L 3.5-5.0mmol/L 2.2-8.3mmol/L 44-80mmol/L 3.0-6.0mmol/L Table 1.3 Haematology. Hb Haematocrit RBC WBC Platelets INR PT APTT ratio 11.3g/dL 0.24 2.75 x 1012/L 7.5 x 109/L 296 x 109/L 1.4 14.4 seconds 1.4 Normal values 11-16g/dL 0.4-0.5 males, 0.37-0.47 females 3.8-4.8 x 1012/L 4-11 x 109/L 150-450 x 109/L 0.9-1.2 11-15 seconds 0.8-1.2 SOE1_SOE1.qxd 19-04-2013 19:25 Page 3 Structured Oral Examination 1 Figure 1.1 Chest X-ray. Figure 1.2 ECG. aVR V1 V4 aVL V2 V5 aVF V3 V6 3 SOE1_SOE1.qxd 19-04-2013 19:25 Page 4 4 The Structured Oral Examination in Clinical Anaesthesia Practice examination papers Examiner’s questions Please summarise the case A 70-year-old male patient, known to have hypertension and ischaemic heart disease, recovering in intensive care following AAA repair, has developed hypotension and hypoxia at 24 hours postoperatively following tracheal extubation. His biochemistry results suggest impaired renal function and hypokalaemia. What is the differential diagnosis? The important causes of postoperative hypotension and hypoxia in this patient can be listed systematically as follows. Cardiovascular system w Myocardial infarction. w Left ventricular failure or congestive cardiac failure. w Arrhythmias such as atrial fibrillation (AF). Respiratory system w w w w Pulmonary embolism. Pleural effusion. Pneumothorax. Transfusion-related acute lung injury (TRALI). Metabolic causes w Electrolyte imbalance. Infection w Severe systemic infection (sepsis). Analgesia-related w High level of epidural blockade. SOE1_SOE1.qxd 19-04-2013 19:25 Page 5 Structured Oral Examination 1 What are the abnormal findings in the ECG? The ECG shows atrial fibrillation as the rhythm is irregularly irregular with absent P waves and the heart rate is approximately 120 bpm. There is left ventricular hypertrophy and left axis deviation suggesting longstanding hypertension. What are the causes of atrial fibrillation (AF)? Cardiac causes w w w w Ischaemic heart disease. Mitral valve disease. Hypertension. Cardiomyopathy. w w w w w w Hypoxia. Acute hypovolaemia. Sepsis. Electrolyte disturbances - potassium, magnesium and phosphate. Pulmonary thromboembolism. Thyrotoxicosis. Non-cardiac causes In this patient the cause of AF is likely to be ischaemic heart disease, pneumonia and an electrolyte imbalance (low potassium). How would you treat fast atrial fibrillation? w Ensure adequate airway and breathing, and administer 100% oxygen. w Establish continuous ECG, blood pressure and pulse oximetry monitoring. w Correct any precipitating factors where possible. w Determine if the patient is stable or not. If the patient is unstable, he should be treated with synchronised DC cardioversion with shocks up to three attempts. If there is no response, intravenous amiodarone 300mg should be administered over 10-20 minutes and the shock repeated if needed, followed by an amiodarone 900mg IV infusion over 24 hours. 5
© Copyright 2026 ExpyDoc