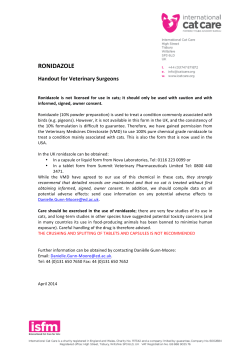
URINARY SATURATION AND UROLITHIASIS Joe Bartges, DVM, PhD, DACVIM (SA IM), DACVN Professor of Medicine and Nutrition The Acree Endowed Chair of Small Animal Research The University of Tennessee Knoxville, TN 37996-4544 [email protected] UROLITH FORMATION Initiation and Growth of Uroliths Urolith formation, dissolution, and prevention involve complex physical processes. Major factors include: 1) supersaturation resulting in crystal formation, 2) effects of inhibitors of crystallization and inhibitors of crystal aggregation and growth, 3) crystalloid complexors, 4) effects of promoters of crystal aggregation and growth, and 5) effects of non-crystalline matrix.(Finlayson 1978; Coe and Parks 1988; Brown and Purich 1992; Bartges, Osborne et al. 1999) Figure 1. Proposed sequence of events resulting in calcium oxalate urolith formation Ca++ Ca++ Ca++ Oxalate= Oxalate= Ca++ Saturation Supersaturation Ca++ Oxalate= Ca++ Ca++ Oxalate= Oxalate= Nucleation Crystal aggregation and growth Crystal retention Stone formation Urolith formation is associated with two complementary but separate phases: initiation and growth. It appears that initiating events are not the same for all types of uroliths. In addition, factors that initiate urolith formation may be different from those that allow it to grow. The initial step in formation of a urolith is formation of a crystal nidus (or crystal embryo). This phase of initiation of a urolith formation, called nucleation, is dependent on supersaturation of urine with calculogenic crystalloids. The degree of urine supersaturation may be influenced by the magnitude of renal excretion of the crystalloid, urine pH, and/or crystallization inhibitors or promoters in urine. Non-crystalline proteinaceous matrix substances may also play a role in nucleation in some instances. Three theories have been proposed to explain initiation of lithogenesis.(Erwin 1976; Coe 1981; Smith 1990; Osborne, Bartges et al. 2000) Each theory emphasizes a single factor. The SUPERSATURATIONCRYSTALLIZATION THEORY incriminates excessive supersaturation of urine with urolith-forming crystalloids as the primary event in lithogenesis. In this hypothesis, crystal nucleation is considered to be a physiochemical process involving precipitation of crystalloids from a supersaturated solution. Urolith formation is thought to occur independently of a) preformed matrix or b) crystallization inhibitors. The MATRIX NUCLEATION THEORY incriminates preformed organic matrix (thought to be a mucoprotein with calcium-binding properties) as the primary determinant in lithogenesis. It is based on the assumption that preformed organic matrix forms an initial nucleus that subsequently permits urolith formation by precipitation of crystalloids. The role of organic matrix in lithogenesis has not been defined with certainty; however, the similarity of the overall composition of matrix from human uroliths of various mineral composition supports this hypothesis. The CRYSTALLIZATION-INHIBITION THEORY proposes that reduction or absence of organic and inorganic inhibitors of crystallization are the primary determinant of calcium oxalate and calcium phosphate lithogenesis. This theory is based on the fact that several lithogenic substances in urine are maintained in solution at concentrations significantly higher that is possible in water (in other words, driving forces for crystal precipitation of normally saturated urine are minimized by crystallization inhibitors). Similarly, inhibitors are important in minimizing crystal growth and aggregation. These three theories are not mutually exclusive. In fact, supersaturation of urine with the crystal's components is a prerequisite for each theory of nucleation. Further growth of the crystal nidus is dependent on the following: (1) its ability to remain in the lumen of the excretory pathway of the urinary system; (2) the degree and duration of supersaturation of urine with crystalloids identical or different from that in the nidus; and (3) physical characteristics of the crystal nidus. If they are compatible with other crystalloid; some crystals may align themselves and grow on the surface of others. This is called epitaxial growth. Epitaxy may represent a heterogeneous form of nucleation, and may account for mixed and compound uroliths. For example, in man, the structural similarities of uric acid and calcium oxalate permit urolith growth by epitaxis. States of Urinary Saturation An important driving force behind stone formation is saturation state of urine with lithogenic substances (Figure 2). When a solution such as urine is saturated, it refers to the maximal amount of a substance, such as calcium oxalate, that can be completed dissolved. This point is termed the thermodynamic solubility product. When calcium oxalate is present in urine at a concentration less than the solubility point, the urine is undersaturated with calcium oxalate and calcium oxalate completely dissociates and dissolves. When calcium oxalate is present in urine at a concentration that is equal to the solubility point, the urine is saturated with calcium oxalate and calcium oxalate begins to precipitate. When calcium oxalate is present in urine at a concentration above the solubility point, the urine is supersaturated with calcium oxalate and calcium oxalate precipitates. Urine contains ions and proteins that interact and/or complex with calcium and oxalic acid so as to allow them to remain in solution. This explains why calcium and oxalic acid in urine do not normally precipitate to form calcium oxalate crystals. Urine is normally supersaturated with respect to calcium and oxalic acid. But energy is required to maintain this state of calcium and oxalic acid solubility, and, therefore, the urine must constantly "struggle" to maintain calcium and oxalic acid in solution. Thus, urine is described as being metastable, implying varying degrees of instability with respect to the potential for calcium oxalate crystals to form. In this metastable state, new calcium oxalate crystals will not precipitate, but if already present, crystals can be maintained and even grown in size. If the concentration of calcium and oxalic acid is increased, a threshold is eventually reached at which urine cannot hold more calcium and oxalic acid in solution. The urine concentration at which this occurs is the formation point of calcium oxalate. Above the thermodynamic formation product, urine is oversaturated and unstable with respect to calcium and oxalic acid. Thus, calcium oxalate crystals will spontaneously precipitate, grow in size, and aggregate together. Figure 2. States of urinary saturation(Bartges, Osborne et al. 1999) Undersaturated Solution An undersaturated solution is one that contains a sufficiently low concentration of a crystalloid to permit dissolution of additional quantities of the crystalloid. Urine is undersaturated when the solute concentration (or activity product) is below the solubility of the solute in question. Creation of urine which is undersaturated with calculogenic crystalloids may permit varying degrees of urolith dissolution. Saturated Solution A saturated solution is one in equilibrium with the un-dissolved solute at a given temperature. The solution contains so much dissolved substance, that no more can be dissolved at a given temperature. With respect to urine, the saturation concentration is the concentration of a crystalloid in urine at which the urine can be mixed with uroliths (or the solid phase) of that crystalloid without changing the concentration of the crystalloid in urine. The saturation of salts in urine is influenced by several variables including pH, ionic strength, and temperature. Supersaturated Solution A supersaturated solution is one which is more saturated with a substance at a given temperature than would be normally expected. In other words, it is any concentration greater than the saturation concentration. Supersaturated urine contains a greater concentration of a crystalloid (cystine, phosphate, calcium, ammonium, etc.) than the associated solvent (water) would be predicted to be able to normally hold in solution. Supersaturation can vary in degree. At lower levels of supersaturation, urine is metastable. At higher levels of supersaturation, however, urine becomes unstable with regard to its capacity to keep crystallogenic substances in solution. Factors that increase the saturation of crystalloids in urine predispose to precipitation of crystals and thus urolith formation. Spontaneous precipitation will occur if the concentration of the crystalloid is greater than the formation product of the crystalloid. Metastable Region The metastable region refers to the degree of supersaturation of a crystalloid that lies between the solubility product and the formation product. Metastability applies to those solutions (such as urine) that have the capacity to retain more of a compound in solution than would be predicted by knowledge of its true solubility in water. The term "metastable" is appropriate because it implies a condition subject to change. A metastable solution is thermodynamically unstable, but does not contain enough energy to initiate crystal formation. However, if crystals are already present, they may grow. The region of metastability varies with the type of calculogenic crystalloid. It has been estimated that the difference between the solubility product and the formation product of calcium oxalate in urine is a multiple of about 8.5 to 10.0. Oversaturated Solution An over-saturated solution is one in which the degree of supersaturation of a crystalloid is greater than the formation product. Recall that supersaturated urine exceeds the solubility product, but does not exceed the formation product. Oversaturated urine is no longer metastable. Nucleation will take place in absence of heterogeneous factors. It is thought that crystals observed by microscopic examination or urine sediment are caused by oversaturation of urine. Nucleation Nucleation refers to the initial event in the formation (or precipitation) of uroliths and is characterized by the appearance of submicroscopic molecular aggregates of crystalloids. Initially, the aggregates are approximately 100 molecules in size and represent potential crystal embryos (or a nidus). Crystals represent an orderly arrangement of atoms in a periodic pattern or lattice. To become a urolith, crystal embryos must have a lattice arrangement that allows continued growth. They must also be large enough to prevent dispersion back into the dissolved phase.(Brown, Ackermann et al. 1994) Nucleation has been classified as homogeneous (also called self nucleation or generalized nucleation) or heterogeneous (also called localized nucleation). Homogeneous nucleation occurs spontaneously in highly supersaturated urine in the absence of foreign substances. Therefore, the nidus is composed of identical crystalloids. Heterogeneous nucleation is catalyzed by foreign material such as suture material, indwelling catheters, tissue debris, crystal embryos of different composition, and so on (Figure 3). Urine contains many impurities that might promote heterogeneous nucleation and initiate crystal formation at a concentration of crystalloids below the formation concentration. These substances may be thought of as facilitators or potential facilitators of crystallization. Any crystal type may be a potential nidus for nucleation of another crystal type. A greater degree of supersaturation (that is, a higher formation product) is required for homogeneous nucleation than for heterogeneous nucleation. Once nucleation has occurred, however, crystal growth can occur at any degree of supersaturation (even at metastability). Figure 3. Example of (a) homogeneous nucleation and (b and c) heterogeneous nucleation. (a) Ammonium urate urolith removed from a 3-year-old, intact male, English bulldog. Note the laminations. (b) Compound urolith removed from a 4-year-old, spayed female Miniature schnauzer. The outer layers are composed of infectioninduced struvite (S) around a calcium oxalate nidus (C). (c) Infection-induced struvite removed from a 2-year-old, spayed female Miniature schnauzer. The urolith (S) formed around a piece of fibrous material (gauze sponge, G) inadvertently left behind at a previous cystotomy for urolith removal. (a) (b) C (c) G S S Inhibitors and Promoters of Crystal Formation Urine is a complex solution containing a variety of substances that can inhibit or promote crystal formation and growth.(Ryall 1997; Dussol and Berland 1998; Kavanagh, Jones et al. 1999; Shirane, Kurokawa et al. 1999; Marangella, Bagnis et al. 2004; Guerra, Meschi et al. 2006; Kumar and Lieske 2006; Jaggi, Nakagawa et al. 2007; Vella, Karydi et al. 2007) Inhibitors include molecules that reduce calcium oxalate and calcium phosphate supersaturation. Some inhibitors (e.g., citrate, magnesium, pyrophosphate) form soluble salts with calcium, oxalic acid or phosphate, and thereby reduce the quantity of calcium, oxalate or phosphate available for precipitation. Other inhibitors (e.g. nephrocalcin, uropontin, glycosaminoglycans, Tamm-Horsfall glycoprotein, other inert ions) interfere with the ability of calcium and oxalic acid to combine, and thereby minimize crystal formation and growth. Also, glycosaminoglycans act as protectors by preventing adherence of crystals to the urinary tract mucosa. METHODS FOR EVALUATING RISK OF UROLITH FORMATION Various factors involved with urolith formation may be evaluated by several methods including: 1) epidemiological studies performed at urolith centers and designed to identify risk and protective factors, 2) measuring urine concentrations of calculogenic substances, 3) evaluating the influence of urine pH on crystal formation, and 4) measuring the degree of undersaturation, supersaturation, and/or oversaturation of urine with crystallogenic substances. Determination of urinary biochemical parameters and urinary saturation can only be done in patients that are “stone free” because active urolith disease results in depletion of calculogenic compounds in urine that alters results.(Laube, Pullmann et al. 2003) An emphasis of urolithiasis research is evaluation of crystallization methods as urolith formation is preceeded and advanced with crystal formation. “ Crystallization is a physical chemical process involving a change of state from solution to solid. The supersaturation, which is a measure of the chemical energy available for this process, is a crucial factor and governs all aspects of crystallization such as nucleation, growth, and aggregation. As the reaction proceeds, the supersation will decline (unless replenished) and this in turn will impact upon the kinetic behavior of the crystallization process. While the physical chemistry and kinetics are always important, the process of stone formation takes place in a biological environment. – JP Kavanagh, 2006(Kavanagh 2006) In addition to various techniques developed to evaluate crystallization, several “risk formulae” have been proposed to evaluate propensity for urolith recurrence (primarily for calcium oxalate) in human patients,(Tiselius 1997) although debate exists as to the utility of these formulae.(Sutton 2006) These include: the urinary calcium-tomagnesium ratio, the urinary calcium-to-citrate ratio, saturation-inhibition index, 24-hour urine quotients [(calcium x oxalate / magensium x creatinine) and (calcium x oxalate / magensium x creatinine x inhibitioin of calcium oxalate crystal growth in dilute urine)], probability index, and the ion-activity product index.(Tiselius 1997) Supersaturation In solution chemistry, the difference in chemical potential of 2 states (Δµ) is dependent on the activities of the crystallizing salt in the supersaturated solution (a) and in the solution when it has come to equilibrium (aeq): Δµ = RTln(a/aeq) where R is the universal gas constant and T is the absolute temperature (Kelvin). The activity of the crystallizing salt is represented by the activity product (AP) for that salt where the activities of the ions comprising that salt are multiplied. The term "activity" of a mineral is an index of the likelihood that the mineral will combine with other substances in urine, and is determined by multiplying the concentration of the ion by the activity coefficient for similarly charged molecules. For example, the activity of calcium is determined by multiplying the concentration of calcium in solution (molarity) by the activity coefficient for a doubly charged molecule since calcium carries a “2+” charge. The "activity" of a mineral is dependent on several factors including: 1) the urine concentration of that mineral, 2) the urine concentrations of other substances such as sodium, potassium, calcium, etc., 3) the quantity and functional state of non-mineral or non-measured mineral inhibitors and promoters of crystal formation, growth, and aggregation, 4) urine pH, and 5) temperature of urine. Thus, a and aeq represent the AP’s for the salt in supersaturated solution and the solution at equilibrium, respectively. Furthermore, the supersaturation ratio (S) = a/aeq; therefore, Δµ/RT = ln(S).(Werness, Brown et al. 1985) For practical purposes, S is expressed as concentrations (molarities) or activities (a). For example, for calcium oxalate: S= APcaox = [Ca2+]x[Ox2-] APcaoxeq [Ca2+eq]x[Ox2-eq] where “[ ]” represents the activities or concentrations of the ions, calcium (Ca2+) or oxalate (Ox2-). Usually, the relative supersaturation (σ) is used rather than S, where σ = S–1.(Finlayson and Miller 1969; Finlayson 1978; Werness, Brown et al. 1985; Brown, Ackermann et al. 1994; Kavanagh 2006) Crystallization involves nucleation, growth, and aggregation. Nucleation may be heterogeneous (where a foreign substance provides a nucleation catalyst for crystal formation) or homogeneous (where no foreign substance is used). Supersaturation required for homogeneous nucleation is much higher than that required for heterogeneous nucleation. There is still a supersaturation barrier that must be overcome before nucleation can occur (Figure 2). Growth of crystals may occur through enlargement of existing crystals by direct incorporation of solution species into the solid crystal lattice or by aggregation of crystals. The rate of crystal growth is described by second order kinetics: G = kσ2 where G is the growth rate and k is the rate constant.(Kavanagh 2006) Aggregation can also result in enlargement of the crystal mass, and occurs through the net result of crystals colliding and either dispersing or consolidating, with the outcome being depending on an efficiency factor. As consolidation is achieved by crystal bridges that fuse the lattice structures of individual crystals, aggregation also is dependent on supersaturation.(David, Espitalier et al. 2001; Hounslow, Mumtaz et al. 2001) There are several techniques used to evaluate urinary saturation. The most commonly used are determination of relative supersaturation and activity product ratios. Relative supersaturation Determining the relative supersaturation (RSS) of a urolith-forming substance in a patient's urine is one technique used to assess risk of urolith formation.(Pak, Hayashi et al. 1977; Brown and Purich 1992) RSS is determined by measuring urine concentrations of several analytes including ammonium, calcium, chloride, citrate, hydrogen (pH), magnesium, oxalate, phosphate, potassium, and sodium (and possibly cystine, sulfate, uric acid, and other compounds), in urine. These values are then entered into a computer program (EQUIL or SUPERSAT), which calculates the activity coefficients for the various ions and combines the relevant ion concentrations and activity coefficients to produce the activity product (AP). For example, the AP of calcium oxalate is calculated as the mathematical product of the activity of calcium and activity of oxalic acid. The AP for each urolith-forming compound is divided by its known thermodynamic solubility product (SP) and the resultant RSS produced. RSS = ion AP of the patient’s urine / ion SP Relative supersaturation is related to the energy available for crystal nucleation and growth; however, RSS values are limited by the fact that the thermodynamic solubility products used for these calculations have not been measured in the patient's urine. This is of concern because it is probable that different macromolecules, including inhibitors and promoters of crystal formation, growth, and aggregation, in the patient's urine have a pronounced influence on free ion concentrations. By using calculations measured in urine from healthy human beings, RSS may overestimate SP’s and AP’s of different minerals, and thus tend to underestimate the risk of urolith formation. Another technical problem in evaluating dogs and cats is that the computer program used to calculate RSS involves comparison of the pet’s urine values to standardized values based on the composition of human urine. Activity product ratios Activity product ratios (APR) also are designed to express the degree of supersaturation of solutions with calculogenic minerals. APR's are obtained by calculating the ion AP in the patient's urine samples before and after equilibrium with various seed crystals such as calcium oxalate. APR = ion AP of patient’s urine before incubation with seed crystals ion AP of patient’s urine after incubation with seed crystals In determining the APR, the patient’s urine is incubated with preformed seed crystals composed of pure urolith-forming mineral of interest (for example, calcium oxalate). Following incubation for 48-hours with the seed crystals, the urine concentration of the same analytes are measured. The post-incubation concentrations of analytes are then used to calculate a "post-incubation" AP. Dividing the "pre-incubation" AP by the "post-incubation" AP gives the APR for that patient's urine sample. An exact measurement of supersaturation is not obtained by determining APR, but the method provides useful information about the relative increase or decrease of the ion AP in the patient's urine that result from seed crystal growth or seed crystal dissolution. An APR less than one represents undersaturation of urine with the mineral being evaluated An APR equal to one represents saturation of the patient's urine sample. An APR greater than one indicates that the patient's urine sample is supersaturated. APR’s can be calculated for any calculogenic mineral as long as pure seed crystals for that type of mineral are available. Use of APR methodology will not eliminate errors associated with the effect of unknown factors such as crystallization inhibitors or promoters on ion activities; however, since the same urine sample obtained from the patient is analyzed before and then after equilibration with seed crystals (such as calcium oxalate), the same type of error occurs in evaluation of both analyses and therefore the errors cancel. Whereas calculation of RSS can overestimate supersaturation, saturation, and undersaturation, the APR method overestimates undersaturation, underestimates supersaturation, and correctly measures saturation, provided that a sufficient amount of seed crystals have been used. One limitation of APR determination is the assumption that urine has reached the SP for the salt following 48 hours of incubation, which has been shown to be a false assumption in some cases.(Robertson, Jones et al. 2002) Urine may not reach true equilibrium saturation level, particularly when coming from a supersaturated level, presumably due to presence of various inhibitors of crystal growth that slow down the approach to equilibrium. In this instance, when the true RSS is measured following 48 hours of seed incubation, the AP achieved at that point may be 2-3 times higher than the thermodynamic solubility product. The APR calculated at this point, therefore, systematically underestimates the actual level of supersaturation since the denominator (AP/SP) is too large. The opposite may occur when the urine is undersaturated. Other measures of urine saturation There are other techniques for estimating urine saturation in addition to relative supersaturation and activity product ratios. A newer method for evaluating risk of calcium oxalate urolith formation in human beings is use of the Bonn Risk Index (BRI).(Laube, Schneider et al. 2000; Laube, Hergarten et al. 2001; Laube, Hergarten et al. 2004) Supersaturation of urine with respect to a urolith-forming salt is a fundamental pre-requisite of salt precipitation as supersaturation is the thermodynamic driving force behind the process; however, supersaturation alone is not sufficient to induce pathologic salting-out. The BRI uses the ratio calculated from the urinary concentration of ionized calcium and the amount of ammonium oxalate that is titrated to the urine in order to induce a precipitation of calcium oxalate salts. A high BRI value indicates low risk of urolith formation (whereas a low RSS indicates low risk) and a low BRI indicates a high risk of urolith formation (whereas a high RSS indicates high risk). BRI has been shown to correlate with RSS.(Laube, Hergarten et al. 2001) For crystallization to occur in the urinary tract, it is necessary that a correct combination of supersaturation and of factors that inhibit/promote the nucleation process exists. To what extent this propensity for crystallization will actually relate to risk of urolith formation also depends on factors that regulate steps leading from a crystal to a urolith. An advantage of BRI is that fact that all urinary components contribute their effects in their native ratio to the determination. Thus, the BRI includes an imbalance between promoters and inhibitors in the individual’s urine, if an imbalance is present; however, the BRI is a non-specific method with respect to urinary constituents as only the concentration of ionized calcium is measured. Additional urinary chemistry determination may be necessary to fully evaluate the metabolic status of a patient. This technique has not been tested in animals, and the instrument (Urolizer, Raumedic Ag, Munchberg, Germany) is not available in the United States. Use of urinary saturation testing in dogs and cats Limited studies utilizing urine saturation testing has been performed in veterinary medicine, particularly in animals that have formed uroliths (Table 1). Despite the number of studies, very few have been performed in dogs or cats that are urolith-formers and no studies exist that compares estimates of urinary saturation with recurrence rates of uroliths. In dogs, calcium oxalate urolith formation typically occurs when urinary relative supersaturation for calcium oxalate is greater than 10; the metastable zone lies between a relative supersaturation value for calcium oxalate of 1 and 10 to 14.(Stevenson and Rutgers 2006) In cats, calcium oxalate urolith formation typically occurs when urinary relative supersaturation for calcium oxalate is greater than 12; the metastable zone lies between a relative supersaturation value for calcium oxalate of 1 and approximately 12.(Houston and Elliott 2008) Sterile struvite urolith formation in cats typically occurs when urinary relative supersaturation for struvite is greater than 2.5; the metastable zone lies between a relative supersaturation value for struvite of 1 and approximately 2.5.(Houston and Elliott 2008) Urinary supersaturation represents a risk for urolith formation, but as in human beings, there is overlap in values between urolith-forming animals and healthy, non-urolith-forming animals.(Robertson, Peacock et al. 1968; Kavanagh 2006); therefore, other factors are important. Use of urinary saturation studies can provide further information as to mechanisms of urolith formation, screening of animals at risk for urolith formation, and monitoring efficacy of urolith management. CLINICAL APPLICATION TO DOGS AND CATS So what does all of this mean? There are several issues to keep in mind: - Urinary saturation is the most important, but not the only, driving force for crystallization and urolith formation - Several methods exist for estimating urinary saturation; however, none of them adequately describe what is occurring naturally in the biological system (urinary tract) - Determination of relative supersaturation and activity product ratios, while used to estimate urinary saturation, give different results and information. Determination of relative supersaturation is a valuable and reasonably reliable technique for estimating urinary saturation; however, it (a) is heavily influenced by concentration of analytes measured, which, in turn, is influenced by urine volume, and (b) it does not account for urinary constituents that are not measured including the influence of inhibitors. Because it is influenced by urine volume, methods designed to increase urine volume (e.g. feeding canned foods, administration of diuretics, and stimulating water consumption by increased levels of dietary sodium) would be expected to lower the relative supersaturation; however, clinical studies in urolith-forming dogs and cats are lacking.(Stevenson, Hynds et al. 2003; Lulich, Osborne et al. 2005; Hezel, Bartges et al. 2006; Xu, Laflamme et al. 2006; Hezel, Bartges et al. 2007; Xu, Laflamme et al. 2009) Determining activity product ratios do not give an exact estimation of the supersaturation; however, because a patient’s urine is used pre- and post-incubation with seed crystals, this technique does account for unmeasured urinary constituents and the influence of inhibitors. - Medical dissolution of uroliths is accomplished by inducing a state of undersaturation of urine (below the solubility product) with the minerals that formed the uroliths - Medical prevention of uroliths is accomplished by induced a state of undersaturation of urine or at least a state of saturation at the lower end of the metastability limit - Despite use of estimates of urinary saturation, there are no published studies in urolith-forming dogs and cats that validate their use as means to predict urolith recurrence. Until that time, these techniques are useful for formulating diets, but await recurrence data for validation. - Means to decrease urinary saturation include increasing urine volume (“dilution is the solution to pollution”) thereby decreasing the concentrations of calculogenic substances and decreasing dietary intake of calculogenic substances. Despite these measures, these measures do not guarantee prevention of urolith recurrence in all patients demonstrating that urolith formation is a complex process and many questions remain un-answered. Table.1. Summary of studies utilizing relative supersaturation or activity product ratio estimates of urinary saturation in dogs and cats. Data, when available, are presented as average (standard deviation). Dogs Dogs Health status* Healthy Labrador retrievers Healthy Miniature schnauzers Healthy miniature schnauzers, beagles, labrador retrievers Treatment group‡ Maintenance dry dog food adult maintenance canned diet Control diet + liquid potassium citrate Control diet + potassium citrate tablet Test and results# RSScaox = 4.60 (1.66) RSSbr = 0.47 (0.23) RSScaox = 5.31 (1.62) RSSbr = 1.22 (0.31) RSScaox = 1.42 (0.63) RSSmap = 2.59 (1.40) RSScaox = 1.68 (0.83) RSSmap = 3.55 (3.43 RSScaox = 1.24 (0.53) RSSmap = 3.44 (2.63) RSScaox = 4.02 (2.43) RSScaox = 2.83 (2.25) Dogs Healthy beagles Canned ltra-low protein, alkalinizing diet (0.24% DM) Above diet + 1.2% NaCl DM Dogs Healthy Labrador Retrievers Maintenance dry dog food Maintenance dry dog food + water Maintenance dry dog food + 0.05 g NaCl/100kcal) Maintenance dry dog food + 0.2 g NaCl/100 kcal Maintenance dry dog food + 0.3 g NaCl/100 kca Maintenance dry dog food Maintenance dry dog food + water Maintenance dry dog food + 0.05 g NaCl/100kcal) Maintenance dry dog food + 0.2 g NaCl/100 kcal Maintenance dry dog food + 0.3 g NaCl/100 kcal l Low calcium (0.18), low oxalate (10)dry diet Low calcium (0.18), medium oxalate (17.5) dry diet Low calcium (0.18), high oxalate (25) drydiet Moderate calcium (0.45), low oxalate (10) dry diet Moderate calcium (0.45), moderate oxalate (17.5) dry diet High calcium (0.75), low oxalate (10) dry diet High calcium (0.75), high oxalate (25)dry diet g/100kcal Stone-formers Non-stone-formers Variable diets RSScaox = 11 (6) RSScaox = 9 (7) RSScaox = 9 (4) RSScaox = 5 (3) RSScaox = 3 (3) RSScaox = 14 (3) RSScaox = 9 (5) RSScaox = 15 (9) RSScaox = 10 (6) RSScaox RSS = 6 (3) RSScaox = 2.5 (0.5) RSScaox = 5.2 (4) RSScaox = 4.3 (1) RSScaox = 4 (2) RSScaox = 4 (2) RSScaox = 6 (5.5) RSScaox = 5.8 (3) Stone formers – baseline 1 month 12 months Normal – baseline 1 month Baseline = variable diets 1 and 12 mo = canned oxalate prevent diet Adult Maintenance canned diet RSScaox = 21.4 (15.8) RSScaox = 7.8 (7.1) RSScaox = 5.1 (2.9) RSScaox = 4.1 (2.0) RSScaox = 2.4 (1.4) Healthy Miniature schnauzers Dogs Healthy Cairn terriers and Miniature schnauzers Dogs Various Dogs Various Dogs Healthy beagles Ultra-low protein, canned diet Dogs Healthy beagles Ultra-low protein, canned diet with casein (10.4% DM) Ultra-low protein, canned diet with casein (20.8% DM) Dogs Healthy beagles Canned diet, casein-based (10.8% protein DM) Dry diet, egg-based (9.2% protein DM) Canned diet, chicken-based (11.1% protein DM) Canned diet, chicken and liver-based (10.7% protein DM) RSScaox = 21.4 (15.8) RSScaox = 4.1 (2.0) APRua = 0.05 (0.04) APRnau = 0.04 (0.03) APRau = 0.14 (0.07) APRua = 0.005 (0.003) APRnau = 0.004 (0.003) APRau = 0.03 (0.03) APRua = 0.005 (0.003) APRnau = 0.005 (0.003) APRau = 0.03 (o.009) APRua = 0.02 (0.01) APRnau = 0.03 (0.02) APRau = 0.13 (0.10) APRua = 0.007 (0.006) APRnau = 0.015 (0.012) APRau = 0.036 (0.028) APRua = 0.033 (0.026) APRnau = 0.50 (0.28) APRau = 0.44 (0.33) APRua = 0.007 (0.007) APRnau = 0.042 (0.002) APRau = 0.052 (0.046) APRua = 0.008 (0.006) APRnau = 0.064 (0.075 APRau = 0.15 (0.15) Reference§ (Stevenson and Markwell 2001) EQUIL (Stevenson, Wrigglesworth et al. 2000) SUPERSAT¥ (Lulich, Osborne et al. 2005) EQUIL (Stevenson, Hynds et al. 2003) SUPERSAT¥ (Stevenson, Hynds et al. 2003) SUPERSAT (Stevenson, Robertson et al. 2003) SUPERSAT (Stevenson, Markwell et al. 2002; Stevenson, Blackburn et al. 2004) SUPERSAT (Bartges, Osborne et al. 1995) EQUIL (Bartges, Osborne et al. 1995) EQUIL (Bartges, Osborne et al. 1995) EQUIL Dogs Healthy beagles Ultra-low protein, canned diet + allopurinol (15 mg/kg PO q12h Week 4 Week 8 Dogs Healthy Beagles and Labrador Retrievers Maintenance dry dog food Cats Healthy DSH cats Maintenance canned cat food Cats Healthy Whiskas low pH canned Waltham feline pH control canned Cats Healthy RC Veterinary cats young adult dry PD Feline c/d dry Hill’s hariball control dry Eukanuba low pH/O dry Cats Various – stone formers Diet on which formed stone Canned oxalate preventative diet Cats Healthy Adult Maintenance Canned Diet with 0.4% Na Adult Maintenance Canned Diet with 0.8% Na Adult Maintenance Canned Diet with 1.2% Na Cats Healthy DSH Adult maintenance, dry diet Diet with hydrochlorothiazide (1 mg/kg PO q12h) Cats Healthy DSH Adult maintenance, dry diet Diet with prednisolone (2.2 mg/kg PO q24h) APRua = 0.01 (0.006) APRnau = 0.02 (0.013) APRau = 0.32 (0.27) APRxan = 0 (0) APRua = 0.003 (0.003) APRnau = 0.004 (0.002) APRau = 0.03 (0.02) APRxan = 0.26 (0.09) APRua = 0.005 (0.003) APRnau = 0.009 (0.004) APRau = 0.088 (0.051) APRxan = 0.27 (0.12) RSScaox = 1.21 (0.03) S RSScaox = 1.52 (0.03) E RSSmap = 1.48 (0.25) S RSSmap = 6.61 (1.17)E RSScaox = 0.97 (0.03) S RSScaox = 1.14 (0.03) E RSSmap = 1.35 (0.15) S RSSmap = 5.74 (0.58) E RSSmap = 0.16 (0.14) RSScaox = 0.37 (0.24) RSSmap = 0.58 (0.18) RSScaox = 0.45 (0.16) APRcaox = 1.11 (0.19) APRmap = 0.72 (0.28) APRcaox = 1.20 (0.23) APRmap = 0.32 (0.06) APRcaox = 1.21 (0.23) APRmap = 0.66 (0.34) APRcaox = 1.25 (0.22) APRmap = 0.91 (0.2) RSScaox = 14.3 (8.4) APRcaox = 3.86 (1.59) RSScaox = 5.9 (1.9) APRcaox = 2.01 (0.59 RSScaox = 4.04 ((2.04) APRcaox = 6.30 (13.69) RSSmap = 0.06 (0.04) APRmap = 1.26 (0.51) RSScaox = 2.97 (2.04) APRcaox = 4.76 (3.69) RSSmap = 0.06 (0.04) APRmap = 1.13 (0.51) RSScaox = 2.52 (2.04) APRcaox = 4.20 (3.69) RSSmap = 0.1 (0.04) APRmap = 0.79 (0.51) RSScom = 3.48 (1.12) RSScod = 1.49 (0.46) RSSmap = 3.82 (2.30) RSScom = 1.12 (0.70) RSScod = 0.48 (0.30) RSSmap = 1.35 (0.05) RSScom = 0.36 (0.33) RSScod = 0.47 (0.38) RSSmap = 0.38 (0.32) RSScom = 0.62 (0.42) RSScod = 0.49 (0.40) RSSmap = 1.59 (0.88) (Bartges, Osborne et al. 1994) EQUIL (Robertson, Jones et al. 2002) SUPERSAT AND EQUIL (Markwell, Smith et al. 1999) EQUIL (Devois, Biourge et al. 2000) EQUIL (Lulich, Osborne et al. 2004) EQUIL (Xu, Laflamme et al. 2006) EQUIL (Hezel, Bartges et al. 2007) EQUIL (Geyer, Bartges et al. 2007) EQUIL Cats Healthy DSH Commercial adult maintenance, dry foods: A B C D E F G H I Cats Healthy Purified adult maintenance diet Purified diet with 0.45% MgCl Purified diet with 0.45% MgOxide Adult maintenance canned diet Adult struvite preventative canned diet RSScaox = 2.96 (0.68) RSSmap = 19.12 (5.42) RSScaox = 5.66 (0.91) RSSmap = 4.08 (1.36) RSScaox = 5.40 (0.91) RSSmap = 3.22 (1.23) RSScaox = 6.52 (1.9) RSSmap = 2.85 (1.43) RSScaox = 2.88 (1.69) RSSmap = 2.98 (2.22) RSScaox = 1.30 (0.52) RSSmap = 1.63 (1.14) RSScaox = 3.68 (2.09) RSSmap = 0.85 (0.69) RSScaox = 3.47 (1.59) RSSmap = 12.18 RSScaox = 2.32 (1.15) RSSmap = 0.75 (0.37) pSAPcalc = 9.18 (0.83) pSAPEQUIL = 10.76 (0.65) pSAPcalc = 11.40 (0.24) pSAPEQUIL = 12.10 (0.24) pSAPcalc = 7.80 (0.91) pSAPEQUIL = 10.21 (0.60) pSAPcalc = 10.78 (0.38) pSAPEQUIL = 11.61 (0.28) pSAPcalc = 10.11 (0.66) pSAPEQUIL = 11.32 (0.38) pSAP = 9.07 (0.34) pSAP = 9.91 (0.34) Cats Healthy Dry diet with 29% protein DM corn gluten and fish meal Dry diet with 55% protein DM corn gluten and fish meal Cats Healthy Dry diet with 32.6% protein as meat meal Dry diet with 32.5% protein as corn gluten meal pSAP = 10.17 (0.34) pSAP = 10.11 (0.34) Cats Healthy Cats Healthy Adult dry diet with 39% protein DM as meat meal Adult dry diet with 39% protein DM as chicken meal Adult dry diet with 39% protein DM as corn gluten meal Dry diet (72% protein, 7.5% fat, 14% NFE, 0.4% fiber DM) Dry diet (52% protein, 9% fat, 32% NFE, 0.8% fiber DM) Dry diet (52% protein, 14% fat, 25% NFE, 3.3% fiber DM) Diets as above, but daily intake normalized for protein Dry diet (72% protein, 7.5% fat, 14% NFE, 0.4% fiber DM) Dry diet (52% protein, 9% fat, 32% NFE, 0.8% fiber DM) Dry diet (52% protein, 14% fat, 25% NFE, 3.3% fiber DM) Adult dry diet with 29% protein DM Adult dry diet with 55% protein DM Adult dry diet with 29% protein DM Same diet with 1.5% ammonium chloride Same diet with 0.75% sodium chloride Adult maintenance dry diet Diet with 1% d,l-methionine Diet with 2% d,l-methionine Experimental diet with 27% protein DM Experimental diet with 1.5% ammonium chloride Adult maintenance canned diet pSAP = 9.27 (0.31) pSAP = 9.20 (0.31) pSAP = 9.61 (0.52) pSAP = 9.45 (0.38) pSAP = 9.04 (0.55) pSAP = 9.29 (0.42) Cats Healthy Cats Healthy Cats Healthy Diet + 0.1 mg/BWkg takushya Diet + 0.5 mg/BWkg choreito Cats Healthy Adult maintenance canned diet Same diet with 0.25 gm/BWkg chorieto Same diet with 0.5 gm/BWkg chorieto Same diet with 1 gm/BWkg chorieto Same diet with 2 gm/BWkg chorieto Same diet with 4 gm/BWkg chorieto pSAP = 9.48 (0.39) pSAP = 9.05 (0.45) pSAP = 8.99 (0.39) pSAP = 9.08 (0.68) pSAP = 9.71 (0.63) pSAP = 8.81 (0.45) pSAP = 9.00 (0.73) pSAP = 10.56 (0.66) pSAP = 9.71 (1.13) pSAP = 9.46 (1.13) pSAP = 10.61 (1.13) pSAP = 8.43 (3.04) pSAP = 9.65 (3.04) RSSmap = 5.70 (4.74) pSAPmap = 9.52 (0.44) RSSmap = 3.47 (2.02) pSAPmap = 9.76 (0.45) RSSmap = 2.53 (2.56) pSAPmap = 9.92 (0.44) pSAP = 8.5 (0.3) pSAP = 8.9 (0.3) pSAP = 9.2 (0.6) pSAP = 9.2 (0.6) pSAP = 9.3 (0.4) pSAP = 9.4 (0.2) (Smith, Stevenson et al. 1998) EQUIL (Buffington, Rogers et al. 1990) Hand calculated or EQUIL (Funaba, Hashimoto et al. 1996) Hand calculated (Funaba, Matsumoto et al. 2002) Hand calculated (Funaba, Oka et al. 2005) Hand calculated (Funaba, Uchiyama et al. 2004) Hand calculated (Funaba, Yamate et al. 2003) Hand calculated (Funaba, Yamate et al. 2001) Hand calculated (Buffington, Blaisdell et al. 1997) EQUIL (Buffington, Blaisdell et al. 1992) Cats Healthy Adult maintenance dry struvite preventative diet Adult maintenance canned struvite preventative diet Adult maintenance dry high fiber diet Adult maintenance canned high fiber diet APRmap = 0.47 (0.31) APRcaox = 2.51 (1.15) APRmap = 0.68 (0.29) APRcaox = 1.43 (1.27) APRmap = 0.84 (0.49) APRcaox = 2.21 (0.90) APRmap = 1.98 (0.96) APRcaox = 0.52 (0.30) (Bartges, Tarver et al. 1998) * Healthy – non-urolith-forming animals, DSH = domestic short-hair ‡ NFE = nitrogen free extract # RSScaox = relative supersaturation for calcium oxalate, APRcaox = activity product ratio for calcium oxalate, RSSmap = relative supersaturation for struvite (magnesium ammonium phosphate), APRmap = activity product ratio for struvite, RSScom = relative supersaturation for calcium oxalate monohydrate, RSScod = relative supersaturation for calcium oxalate dihydrate, RSSbr = relative supersaturation for brushite, APRua = activity product ratio for uric acid, APRnau = activity product ratio for sodium urate, APRau = activity product ratio for ammonium urate, APRxan = activity product ratio for xanthine, pSAP = negative logarithm of struvite activity product where pSAP is negatively related to struvite crystal formation. § EQUIL = EQUIL program (various versions), College of Medicine, University of Florida, SUPERSAT = SUPERSAT program, Dr. W.G. Robertson. ¥ Values are approximate based on figure in manuscript; results were not included in table in text REFERENCES Bartges, J. W., C. A. Osborne, et al. (1995). "Influence of four diets containing approximately 11% protein (dry weight) on uric acid, sodium urate, and ammonium urate urine activity product ratios of healthy beagles." Am J Vet Res 56(1): 60-5. Bartges, J. W., C. A. Osborne, et al. (1995). "Diet effect on activity product ratios of uric acid, sodium urate, and ammonium urate in urine formed by healthy beagles." Am J Vet Res 56(3): 329-33. Bartges, J. W., C. A. Osborne, et al. (1995). "Influence of two amounts of dietary casein on uric acid, sodium urate, and ammonium urate urinary activity product ratios of healthy beagles." Am J Vet Res 56(7): 893-7. Bartges, J. W., C. A. Osborne, et al. (1994). "Influence of chronic allopurinol administration on urine acivty product ratios of uric acid, sodium urate, ammonium urate, and xanthine." J Vet Intern Med 8: 168A. Bartges, J. W., C. A. Osborne, et al. (1999). "Methods for evaluating treatment of uroliths." Vet Clin North Am Small Anim Pract 29(1): 45-57. Bartges, J. W., S. L. Tarver, et al. (1998). Comparison of struvite activity product ratios and relative supersaurations in urine collected from healthy cats consuming four struvite management diets. Ralston Purina Nutrition Symposium, St. Louis, MO. Brown, C. and D. Purich (1992). Physical-chemical processes in kidney stone formation. Disorders of Bone and Mineral Metabolism. F. Coe and M. Favus. New York, Raven Press: 613-624. Brown, C. M., D. K. Ackermann, et al. (1994). "EQUIL 93: a tool for experimental and clinical urolithiasis." Urol Res 22: 119-126. Buffington, C. A., J. L. Blaisdell, et al. (1992). "Effect of choreito on struvite solubility in cats." Feline Practice 20(6): 13-17. Buffington, C. A., J. L. Blaisdell, et al. (1997). "Effects of choreito and takushya consumption on in vitro and in vivo struvite solubility in cat urine." Am J Vet Res 58(2): 150-2. Buffington, C. A., Q. R. Rogers, et al. (1990). "Effect of diet on struvite activity product in feline urine." Am J Vet Res 51(12): 2025-30. Coe, F. and J. Parks (1988). Nephrolithiasis: Pathogenesis and Treatment. Chicago, Year Book Medical Publishers Inc. Coe, F. L. (1981). "Nephrolithiasis: causes, classification, and management." Hosp Pract (Hosp Ed) 16(4): 33-45. Devois, C., V. Biourge, et al. (2000). Struvite and oxalate activity product ratios and crystalluria in cats fed acidifying diets. Urolithiasis 2000, Capetown, South Africa. Dussol, B. and Y. Berland (1998). "Urinary kidney stone inhibitors. What is the news?" Urol Int 60(2): 69-73. Erwin, D. T. (1976). "Nephrolithiasis: recent advances in therapy." South Med J 69(7): 935-7. Finlayson, B. (1978). "Physiochemical aspects of urolithiasis." Kidney Int 13: 344-360. Funaba, M., M. Hashimoto, et al. (1996). "Effects of a high-protein diet on mineral metabolism and struvite activity product in clinically normal cats." Am J Vet Res 57(12): 1726-32. Funaba, M., C. Matsumoto, et al. (2002). "Comparison of corn gluten meal and meat meal as a protein source in dry foods formulated for cats." Am J Vet Res 63(9): 1247-51. Funaba, M., Y. Oka, et al. (2005). "Evaluation of meat meal, chicken meal, and corn gluten meal as dietary sources of protein in dry cat food." Can J Vet Res 69(4): 299-304. Funaba, M., A. Uchiyama, et al. (2004). "Evaluation of effects of dietary carbohydrate on formation of struvite crystals in urine and macromineral balance in clinically normal cats." Am J Vet Res 65(2): 138-42. Funaba, M., T. Yamate, et al. (2003). "Effects of a high-protein diet versus dietary supplementation with ammonium chloride on struvite crystal formation in urine of clinically normal cats." Am J Vet Res 64(8): 1059-64. Funaba, M., T. Yamate, et al. (2001). "Effect of supplementation of dry cat food with D,L-methionine and ammonium chloride on struvite activity product and sediment in urine." J Vet Med Sci 63(3): 337-9. Geyer, N., J. W. Bartges, et al. (2007). "Influence of prednisolone on urinary calcium oxalate and struvite relative supersaturation in healthy young adult female domestic shorthaired cats." Vet Ther 8(4): 239-46. Guerra, A., T. Meschi, et al. (2006). "Concentrated urine and diluted urine: the effects of citrate and magnesium on the crystallization of calcium oxalate induced in vitro by an oxalate load." Urol Res. Hezel, A., J. W. Bartges, et al. (2006). "Influence of hydrochlorothiazide on urinary calcium oxalate relative supersaturation in healthy adult cats." J Vet Intern Med 20(3): 741. Hezel, A., J. W. Bartges, et al. (2007). "Influence of hydrochlorothiazide on urinary calcium oxalate relative supersaturation in healthy young adult female domestic shorthaired cats." Vet Ther 8(4): 247-54. Jaggi, M., Y. Nakagawa, et al. (2007). "Tamm-Horsfall protein in recurrent calcium kidney stone formers with positive family history: abnormalities in urinary excretion, molecular structure and function." Urol Res 35(2): 55-62. Kavanagh, J. P. (2006). "In vitro calcium oxalate crystallisation methods." Urol Res 34(2): 139-45. Kavanagh, J. P., L. Jones, et al. (1999). "Calcium oxalate crystallization kinetics at different concentrations of human and artificial urine, with a constant calcium to oxalate ratio." Urol Res 27(4): 231-7. Kumar, V. and J. C. Lieske (2006). "Protein regulation of intrarenal crystallization." Curr Opin Nephrol Hypertens 15(4): 374-80. Lulich, J. P., C. A. Osborne, et al. (2004). "Effects of diet on urine composition of cats with calcium oxalate urolithiasis." J Am Anim Hosp Assoc 40(3): 185-91. Lulich, J. P., C. A. Osborne, et al. (2005). "Effects of dietary supplementation with sodium chloride on urinary relative supersaturation with calcium oxalate in healthy dogs." Am J Vet Res 66(2): 319-24. Marangella, M., C. Bagnis, et al. (2004). "Crystallization inhibitors in the pathophysiology and treatment of nephrolithiasis." Urol Int 72 Suppl 1: 6-10. Markwell, P. J., B. H. E. Smith, et al. (1999). "A non-invasive method for assessing the effect of diet on urinary calcium oxalate and struvite relative supersaturation in the cat." Anim Tech 50(2): 61-7. Osborne, C. A., J. W. Bartges, et al. (2000). Canine urolithiasis. Small Animal Clinical Nutrition. M. S. Hand, C. D. Thatcher, R. L. Remillard and P. Roudebush. Marceline MO, Wadsworth Publishing Co: 605-688. Robertson, W. G., J. S. Jones, et al. (2002). "Predicting the crystallization potential of urine from cats and dogs with respect to calcium oxalate and magnesium ammonium phosphate (struvite)." J Nutr 132(6 Suppl 2): 1637S-41S. Ryall, R. L. (1997). "Urinary inhibitors of calcium oxalate crystallization and their potential role in stone formation." World J Urol 15(3): 155-64. Shirane, Y., Y. Kurokawa, et al. (1999). "Study of inhibition mechanisms of glycosaminoglycans on calcium oxalate monohydrate crystals by atomic force microscopy." Urol Res 27(6): 426-31. Smith, B. H., A. E. Stevenson, et al. (1998). "Urinary relative supersaturations of calcium oxalate and struvite in cats are influenced by diet." J Nutr 128(12 Suppl): 2763S-2764S. Smith, L. H. (1990). "The pathophysiology and medical treatment of urolithiasis." Semin Nephrol 10(1): 31-52. Stevenson, A. E., J. M. Blackburn, et al. (2004). "Nutrient intake and urine composition in calcium oxalate stone-forming dogs: comparison with healthy dogs and impact of dietary modification." Vet Ther 5(3): 218-31. Stevenson, A. E., W. K. Hynds, et al. (2003). "Effect of dietary moisture and sodium content on urine composition and calcium oxalate relative supersaturation in healthy miniature schnauzers and labrador retrievers." Res Vet Sci 74(2): 145-51. Stevenson, A. E., W. K. Hynds, et al. (2003). "The relative effects of supplemental dietary calcium and oxalate on urine composition and calcium oxalate relative supersaturation in healthy adult dogs." Res Vet Sci 75(1): 33-41. Stevenson, A. E. and P. J. Markwell (2001). "Comparison of urine composition of healthy Labrador retrievers and miniature schnauzers." Am J Vet Res 62(11): 1782-6. Stevenson, A. E., P. J. Markwell, et al. (2002). "The effect of diet on calcium oxalate urinary relative supersaturation (RSS) of stone-forming (SF) and normal (N) dogs." J Vet Intern Med 16(3): 377. Stevenson, A. E., W. G. Robertson, et al. (2003). "Risk factor analysis and relative supersaturation as tools for identifying calcium oxalate stoneforming dogs." J Small Anim Pract 44(11): 491-6. Stevenson, A. E., D. J. Wrigglesworth, et al. (2000). "Effects of dietary potassium citrate supplementation on urine pH and urinary relative supersaturation of calcium oxalate and struvite in healthy dogs." Am J Vet Res 61(4): 430-5. Sutton, R. A. (2006). "The use of risk indices: do they predict recurrence?" Urol Res 34(2): 122-5. Tiselius, H. G. (1997). "Risk formulas in calcium oxalate urolithiasis." World J Urol 15(3): 176-85. Vella, M., M. Karydi, et al. (2007). "Pathophysiology and clinical aspects of urinary lithiasis." Urol Int 79 Suppl 1: 26-31. Xu, H., D. P. Laflamme, et al. (2006). "Effect of dietary sodium on urine characteristics in healthy adult cats (abstract)." J Vet Intern Med 20(3): 738. Xu, H., D. P. Laflamme, et al. (2009). "Effects of dietary sodium chloride on health parameters in mature cats." J Feline Med Surg 11(6): 435-41.
© Copyright 2026 ExpyDoc