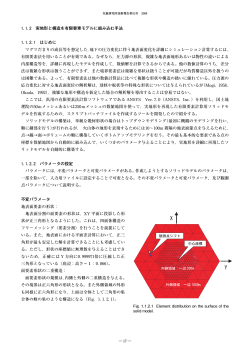
Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Available online at www.ordoneardentistrylibrary.org ISSN 2249-488X Case - report INTERNATIONAL JOURNAL OF RESEARCH IN DENTISTRY MANAGEMENT OF DISCOLORED NON VITAL TEETH WITH ENDODONTIC TREATMENT AND BLEACHING-A CASE REPORT 1 Dr.Puneet Goyal* , Dr.Samriti Bansal1, Dr.Shaveta Bansal2, Dr. Prathibha Garg3 1. Department of Pediatric and Preventive Dentistry, Guru Nanak Dev Dental College and Research Institute, Sunam (Punjab). 2. Department of Prosthodontics, Guru Nanak Dev Dental College and Research Institute Sunam (Punjab). 3. Department of Pediatric and Preventive Dentistry, Guru Nanak Dev Dental College and Research Institute, Sunam (Punjab). Received: 22 Dec. 2013; Revised: 19 Jan 2014; Accepted: 23 Feb. 2014; Available online: 5 Mar 2014 ABSTRACT Modern trends in cosmetic dentistry and media coverage of smile makeovers have increased public awareness of dental aesthetics. Discolored anterior teeth are often perceived as an esthetic detraction. An array of treatment alternatives like ceramics or composite veneering, bleaching, full coverage crowns macroabrasion and microabrasion are available. Bleaching of endodontically treated intact teeth presenting with chromatic alterations is a conservative alternative to a more invasive esthetic treatment such as placement of crowns or veneers. Keywords: Trauma, Tooth discoloration, Triple antibiotic paste, MTA apical plug, Bleaching INTRODUCTION Modern trends in cosmetic dentistry and media coverage of smile makeovers have increased public awareness of dental aesthetics. The ‘first impression’ craze has continually impressed upon the younger generation, the importance of a bright white smile[8]. People now know that smile aesthetics plays a key role in their sense of well-being, social acceptance, success at work and in relationships, and self-confidence. The aesthetic expectations and demands of dental patients have increased substantially. Now, a glowing, healthy and vibrant smile is no longer available only to millionaires and movie stars. Discolored anterior teeth are often perceived as an esthetic detraction[5]. An array of treatment alternatives like ceramics or composite veneering, bleaching, full coverage crowns, macroabrasion and microabrasion are available. Most of these treatment modalities are expensive, need exclusive materials and the need of specialized laboratories.8 Bleaching of endodontically treated intact teeth presenting with chromatic alterations is a conservative alternative to a more invasive esthetic treatment such as placement of crowns or veneers. The 65 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 purpose of this article is to present a brief history of bleaching and a case of discolored non-vital tooth which was successfully bleached using combination technique. Case Report An 11-year-old female patient reported to Department of Pediatric and Preventive Dentistry, with a complaint of discoloration of tooth in the upper front region(fig. I). Patient gave a history of trauma 3 years back to upper front left tooth, following which patient had pain and reported to a private practitioner for the same. Root canal treatment was done but the patient noticed slight change in color of the same tooth which increased gradually. At present, she reported to our department with a complaint of discoloration of tooth . On intraoral examination a severely discolored tooth 21 was found with a fracture involving enamel, dentine and pulp, and no restoration or coronal seal was seen. No abscess or tenderness was found i.r.t 21. IOPA radiograph revealed a poorly condensed obturating material extruding periapically but deficient in cervical half of the root canal. The GP points were seen extruding 3-4mm beyond the apex. There was blunderbuss canal with a periapical radiolucency measuring 4-5 mm in sagittal plane and 3mm in transverse diameter. No cervical erosion or root resorption were seen(fig.II). Treatment plan- Retreatment of tooth included apical seal, obturation, bleaching and final restoration. Retrieval of the extruded obturating material had to be carried out either in orthograde manner or retrograde manner after rasing a periapical flap. Apical plug was planned using MTA followed by obturation and finally bleaching of discolored crown and composite resin restoration of the fractured segment. Debris was cleaned out of the open root canal space with irrigating solutions (5.2% NaOCl and normal saline). Old obturating material was removed in an orthograde manner with the help of d-limonene based Gutta Percha solvent (Carvene ,Prevest). Complete removal of GP points was achieved in orthograde manner, avoiding periapical surgical procedure (fig.III). A frank pus discharge was seen during the procedure, thus cleaning and shaping of the canal followed by placement of triple antibiotic paste was performed. After 3 weeks, periapical radiolucency was reduced and bone deposition was seen in trabecular pattern. Then, MTA apical plug was obtained followed by obturation of the canal space and IRM (Dentsply, Caulk) placement (fig.IV and V). Patient was recalled after 15 days , to find the tooth asymptomatic with no pathological feature. Preoperative shade matching was done with VITA classical shade guide (VITA Zahnfabrik,H.Rauter GmbH and co.,Germany) as C4. After the application of protective cream on the surrounding gingival tissue, the tooth was isolated with rubber dam and the access was re-established by removing IRM .Coronal gutta percha was also removed from canals about 2 mm apical to cervical line. The cavity was irrigated with NaOCl to remove smear layer and debris. A plug of 2 mm thickness of a resin-modified glass ionomer (Vitremer, 3M ESPE) was placed on top of the gutta-percha filling in a shape conforming to the shape of outer CEJ and 1mm incisal to it 66 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 by external probing of the CEJ and epithelial attachment to prevent percolation of bleaching agent into the cervical and apical region. A mixture of sodium perborate and superoxol(30% H2O2) was placed inside the cavity and a gauze piece dampened with superoxol was applied on labial surface to facilitate external bleaching . Then repeated application of heated instrument against dampened gauze was done until the bleach evaporates, taking care that the temperature was less than the patient could tolerate comfortably usually between 50ºC -60ºC. The procedure was continued for five minutes with the gauze being changed every one minute (fig.VI and VII). The bleaching mixture was removed and cavity was rinsed with normal saline. The shade was recorded again (C1)(fig.VIII). A fresh mix of sodium perborate and superoxol as walking bleach was placed in pulp chamber. The excess was removed with dampened cotton and cavity was sealed with IRM to a depth of atleast 3mm to ensure good seal. Patient was recalled after every 7 days to change the Walking bleach paste. After 3 visits, the shade (A2) as desired was obtained (fig.IX). Later, Ca(OH)2 paste along with GIC was sealed for two weeks . After 2 weeks, composite resin build up was done (fig.X). 3 months postoperatively, the tooth is asymptomatic with no change in shade and IOPA revealed decreased periapical radiolucency and no cervical erosion (fig.XI). Discussion This report describes a case where orthograde root canal treatment, retreatment and apexification were done prior to intracoronal bleaching for treatment of a discolored infected maxillary left central incisor before apexification. Persistent or secondary intraradicular infection is a major cause of endodontic failures. Retreatment of poorly obturated root canals is sometimes a necessity in endodontic practice. Over the years, nonsurgical endodontic retreatment has replaced apical surgery as the treatment of choice for cases of endodontic therapy failure. Various techniques are employed to remove gutta-percha, including the use of hand or rotary instruments with or without heat application, solvents, and/or ultrasound. Different solvents have been largely used to empty the root canal. Among them, Orange oil is an excellent alternative solvent as compared to potentially toxic solvents, being used either on eugenol zinc-oxide cement or to soften and dissolve guttapercha. The periapical radiolucency eventually disappeared following orthograde retreatment along with placement triple antibiotic paste. With the present case, the difficulty in obtaining apical stops to enable controlled obturation was overcome by placement of mineral trioxide aggregate (MTA) after interim treatment with an antibacterial agent. Mineral trioxide aggregate (MTA) could be considered for use as an apical plug over the long-term placement of calcium hydroxide, known to stimulate calcific barriers (Heithersay 1975) and exert an antimicrobial action (Stevens & Grossman,1983) because of an advantage of speed at which the treatment can be completed. 67 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Finally bleaching was considered as treatment of choice for management of discolored crown as it improve the appearance of discolored teeth while preserving tooth structure, and it avoids more costly invasive dental treatment. Bleaching is not new!! The earliest effort to lighten teeth through bleaching took place more than a centuries ago, with bleaching agent painted directly on the tooth surface or packed inside a vital tooth. The exact bleaching/whitening mechanism is not fully understood but is thought to involve the ingress of oxidizers and oxygenating molecules via enamel micropores along a diffusion gradient and via direct access of dentine. These are believed to reduce or cause degradation of high molecular weight and complex organic molecules that reflect a specific wavelength of light that is responsible for the color of the stain. The resulting degradation products are of lower molecular weight and composed of less complex molecules that reflect less light, resulting in a reduction or elimination of discoloration. Occurrence of external cervical resorption is a serious complication after internal bleaching procedures. Animal studies have shown histological evidence of resorption after 3 months of bleaching[2]. This is probably caused by the oxidizing agent, particularly 30 to 35% hydrogen peroxide. A postoperative radiograph after bleaching and regular follow -up radiographs are recommended to diagnose possible cervical resorption. According to Hansenbayless and David, as root filling does not adequately prevent diffusion of bleaching agents from the pulpal chamber to the apical foramen, a valid cervical seal is necessary to prevent radicular percolation of bleaching agent. The shape of the cervical barrier should be similar to the external anatomic landmarks, thus reproducing CEJ position and interproximal bone level. The shape from facial view is “bobsled tunnel” outline and proximal outline resembles “skislope”[12]. Application of catalase for three minutes following intracoronal bleaching also eliminates residual hydroxyl ions thus can prevent cervical resorption. Acidulated thio urea is also an effective scavenger of residual hydrogen peroxide and hydroxyl radicals generated during intracoronal bleaching. Conclusion It can be concluded that science of bleaching has become an important and valuable part of esthetic dental arena. It is adjunct in endodontic treatment to get good aesthetic results. Proper diagnosis, selection of bleaching materials, placement technique, and an understanding of the biologic interaction with soft and hard tissues are all factors that determine not only immediate success but also long term success, safety, and patient satisfaction as well. 68 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 REFERENCES 1) Rolly Shrivastava Agarwal, Suparna Ganguly Saha: Inside-Outside bleaching of discolored non-vital teeth. International Journal of Dental Clinics. 2011; 3(3): 95-96. 2) Plotino G, Buono L, Grande NM, Pameijer CH, Somma F: Nonvital tooth bleaching: a review of the literature and clinical procedures. J Endod 2008 Apr; 34(4): 394-407 3) Dahl J.E. and Pallesen U: Tooth Bleaching--a Critical Review of the Biological Aspects. Critical Reviews in Oral Biology & Medicine. 2003; 14(4): 292-304 4) Alyson Wray and Richard Welbury: Treatment Of Intrinsic Discoloration In Permanent Anterior Teeth In Children And Adolescents. International Journal of Paediatric Dentistry 2001; 11(4): 309-315 5) Brigitte Zimmerli, Franziska Jeger, Adrian Lussi: Bleaching of Nonvital Teeth- Clinically Relevant Literature Review. Research and Science 2010: 120(4); 306-313 6) Nagaveni N.B., Umashankara K.V. , Radhika N. B. , Satisha T.S. et al: Management of tooth discoloration in non-vital endodontically treated tooth – A report of 6 year follow-up. J Clin Exp Dent 2011; 3(2): e180-3 7) Anuradha Rani , Manisha Gotarkar : Walking Bleach-still Relevant; A Review With — A Case Report. Indian journal of dental research 2009:1(2); 32-37 8) Pratima Shenoi, Archana Kandhari, Mohit Gunwal: Esthetic enhacement of discolored teeth by macroabrasion and microabrasion and psychological impact on patient-a case series.Indian Journal of Multidisciplinary Dentistry 2012: 2(1) 9) Prasanna Neelakantan, Nithya Jagannathan: Non Vital Bleaching – A Non Invasive Post Endodontic Treatment Option: A Case Report. .Journal of Clinical and Diagnostic Research 2012 May (Suppl-1): Vol-6(3); 527-529 10) M. Sulieman. An Overview of Bleaching Techniques:1: History, Chemistry, Safety and Legal Aspects. Dent Update 2004; 31: 608-616 11) . Ilan Rotstein : Tooth Discoloration And Bleaching. Ingle I.J., Leif K. Bakland. “ Endodontics”, 5th Edn, William & Wilkins, 2003: 845-860. 12) Goldstein R.E,Garber DA.: “Complete Dental Bleaching”, Chicago: Quintessence Publishing Co. Inc; 1995. 13) Greenwall L, Fredman G, Gordan VV. “Bleaching techniques in restorative dentistry: An Illustrated Guide”.New York: Martin Dunitz; 2001. 69 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 PHOTOGRAPHS Fig.I (showing discoloration of tooth 21) Fig.II (. IOPA radiograph revealed a poorly condensed obturating material extruding periapically, deficient in cervical half of the root canal. The GP points were seen extruding 3-4mm beyond the apex. There was blunderbuss canal with a periapical radiolucency ) fig.III (Complete removal of GP points) 70 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 fig.IV fig.V (showing MTA apical plug was obtained followed by obturation of the canal radiolucency) Fig.VI and reduced periapical fig.VII (mixture of sodium perborate and superoxol(30% H2O2) was placed inside the cavity and a gauze piece dampened with superoxol was applied on labial surface to facilitate external bleaching) Fig.VIII[shade was recorded again (C1)]] Fig.IX (. After 3 visits, the shade (A2) as desired was obtained) 71 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014 Fig.X( composite build up done ) fig.XI(after 3 months) 72 Dr.Puneet Goyal et al. / IJRID Volume 4 Issue 1 Jan.-Feb 2014
© Copyright 2026 ExpyDoc