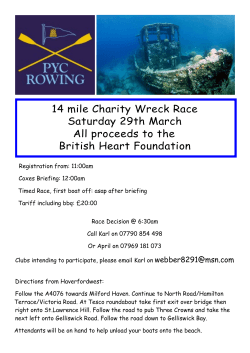
CPD Clinical Articles 5-8 by Dr David Penn Article 5 Article AwAiting cPD Point APProvAl from the DentAl BoArD. clinical Please refer to our website for updates: www.australasiandentist.com.au The Seven Deadly Sins Common errors to avoid when preparing crowns for all ceramic restorations By Dr David Penn BDS MBA 2 2. Bevelled or feather margins My ceramists will not hesitate to tell me that porcelain is a nightmare to fabricate and finish over any bevelled or feather margin. In addition, if it makes it through the laboratory procedures, it has a higher chance of fracturing during try in or at some point after cementation. For optimal strength and fit with any all-ceramic restoration, use only a shoulder preparation (preferred for pressed ceramics and indirect composites) or a definitive chamfer preparation (ideal for all-ceramics built over aluminium oxide or zirconium oxide copings). 1 Figure 1. Why did this fracture occur? Occlusal loading can often be the cause and is often exacerbated by sharp internal line angles which propagate cracks in ceramic copings. 1. Sharp internal line angles Dr David Penn 58 Australasian Dentist Sharp line angles can cause minor to major problems with fitting and seating which result in considerable time loss and frustration for all of us. This is true for any type of restoration, not just all-ceramics. A premature stress fracture occurring at the seating appointment, or worse yet, soon after cementation (Figure 1), can be the costly result of leaving sharp line angles under an all-ceramic or indirect composite restorations. These issues can also cause an erosion of confidence between us and our patients. It is imperative to remember to round all sharp line angles after the rest of the preparation is completed. Use any tapered, fine diamond bur to perform this important procedure or a Sof-lex disk. Figure 2. The margins of this all ceramic crown preparation are well defined and the line angles have been smoothed as much as is practicable. If an old PFM restoration is being replaced with an existing bevelled (metal) margin, and it cannot be modified into a definitive chamfer or shoulder margin, then stay with a PFM as the replacement crown. A wide selection of chamfer and shoulder burs are available which can be used to prepare all-ceramic margins successfully without unwanted bevels. 3 3. the “J” margin One of the dangers in preparing a definitive shoulder or chamfer margin is the unintended creation of a J (or grooved) margin (Figure 3). This occurs when the apex of the diamond passes the edge of the margin and creates a groove inside the margin. If the coping fabrication technique requires scanning, it can lead to inaccuracy in the scan with a resultant poor marginal fit. Possible physical degradation of the die during handling and certain scanning procedures, in tandem with an area of thin porcelain created on this fragile margin, makes a J margin unacceptable. Unfortunately, some of the manufacturers have tried to convince us that any margin will work. This leads to a basic misunderstanding that somehow, the material or the way it is fabricated will make up for a deficiency in the design of the preparation. The fact is, no matter which system is utilized, a certain minimal amount of room is needed to allow for adequate thickness of the underlying coping and the aesthetic layering porcelain. This is especially true in the gingival margin area and cervical third. Many times, our laboratory technicians have to work with chamfers or shoulders that are too shallow or even nonexistent: the resultant crowns can be bulky and far less aesthetic with poor emergence profile. The solution is simply to prepare a deeper, definitive chamfer or shoulder (minimum width 1.2mm) with sufficient axial wall reduction (minimum 1.5 mm). 4 4. incomplete and/or non-uniform shoulder Figure 3. A “J” margin is created when the apex of the chamfer bur passes the edge of the margin, creating a groove. If you use some of the commercially available chamfer diamonds to prepare the margin, one must exercise caution not to exceed a depth into the tooth equal to more than one half of the width of the bur tip. This means an appropriate diameter bur must always be selected to create the chamfer depth desired. If you wish to correct a J margin that has been accidentally created, it can be converted into a modified shoulder margin by reducing the outer lip with an end-cutting bur. Figure 4. End cutting bur (tissue protected) provides well defined chamfers and rounded shoulders which are ideal for all ceramic crowns This problem causes the porcelain in the cervical areas to vary significantly in thickness, with a potential for premature fracture during fabrication, in the process of seating or after cementation. This can also create aesthetic problems when the underlying abutment shade affects the final colour in the thinner areas of porcelain. When pressed ceramics such as e.max or Empress Esthetic are selected as the ceramic of choice, be sure to maximize strength and aesthetics by preparing a complete and uniform 360 degree shoulder with a width of 1.2- to 1.5- mm (butt-joint margin). 5 clinical 5. rough shoulder Taking a little extra time to go back and round any sharp spicules or undulations left on the margins will pay huge dividends. A smooth shoulder will help to ensure an excellent fit and improved aesthetics at the margin. It can also translate into a reduction in the potential for stress fractures upon seating or a delayed fracture after bonding the crown in place. After the shoulder is prepared with a shoulder bur go back with an appropriately sized end-cutting bur and refine the shoulder. With this bur, it can be done quickly and safely without any further undesired removal of axial tooth structure. Figure 6. These preparations on endodontically treated teeth needed to be prepared slightly subgingivally to mask the dark root surface. The margins need to be smoothed to remove the gouge marks from the shoulder bur. 6 Figure 7. A smooth well defined shoulder ideal for all-ceramic restorations has been recorded in this PVS impression 6. inadequate reduction – labially Figure 5. This is a common all ceramic preparation error. The non-uniform nature of the preparation means that the coping and veneering ceramic will be compromised causing a weakness and potential fracture site when loaded. This dreaded sin is very common amongst new graduates or inexperienced crown and bridge operators. I was often guilty of this in my early days: I would spend an inordinate amount of time preparing an exquisite finishing margin but would forget about providing our lab with enough axial wall reduction and hence, adequate room for the coping and veneering ceramic. “Buccal Belly” can easily be overcome by ensuring that a clear line of sight exists from the occlusal aspect of the preparation down to the gingival margin without impingement. Simply placing a mirror to view the axial wall and then envisaging adequate room for the restoration will soon remind you if further reduction is required. Aim for an even 1.5 mm axial wall reduction with smooth walls. Australasian Dentist 59 clinical 7 7. inadequate reduction – occlusally One of the most common dramas we are faced with is under reduction on the occlusal aspect of all ceramic crown preparations which threaten the stress bearing ability of the restoration and bond between the veneering ceramic and underlying restoration. Additionally, preparations do not match the restoration prescribed: for example, Figure 8. The margins of this all ceramic crown preparation are indistinct, sharp line angles exist circumferentially on the occlusal aspect and further occlusal height reduction also needs to be performed. anatomic occlusal reduction should be less emphasized and smoother (not flat) in any CAD/CAM restorations that are physically scanned, such as Procera (Nobel Biocare) or Calypso and need to be sympathetic to the ground in functional occlusion of the surrounding dentition. Reduction (sometimes major) of the incisal edges of opposing mandibular teeth is done far too frequently to “make room” for the lack of maxillary anatomic lingual reduction. If the proper anterior coupling cannot be accomplished with anatomic reduction of the maxillary teeth alone, then one should consider other alternatives, such as an appropriate opening of the occlusal vertical dimension This often involves having an understanding of comprehensive, interdisciplinary restorative dentistry. conclusion The seven deadly sins wreak havoc with the life-spans of all ceramic restorations on a daily basis. At SCDL, we encourage dentists to improve their clinical skills by asking our clinical advisory panel and our laboratory technicians to give meaningful feedback on preparations, tissue-management effectiveness and impressions. If we are open-minded and have a relationship with them that is based on mutual trust, they will be willing to offer us a unique blend of clinical and technical expertise based on their unique experiences and position in dentistry. When dentists encounter problems with their all ceramic work, our clinical team examine every stage of the clinical and lab procedure to try and ascertain the cause of the dilemma. The solution is often as simple as taking the time to understand the limitations of each material and collectively apply a greater attention to detail and concentrating on avoiding these seven deadly sins. u CPD Questionnaire 1. Bevelled margins are acceptable for pressed ceramic restorations True/False 2. Porcelain fused to Zirconia crowns need less occlusal reduction as the copings are so strong True/False 3. “J” shaped margins are a problem for preparations that are scanned True/False 4. Preparations for all ceramic restorations should be smoothed with sandpaper discs where possible True/False 60 Australasian Dentist 5. Modern day bonding procedures with all ceramic crowns diminish the problems caused by sharp internal line angles True/False 6. End cutting burs help to define and smooth rough margins True/False 7. Shoulders with an internal right angle are more suitable than chamfers for all ceramic restorations True/False 8. Under prepared labial axial walls should be overcome by over contouring the crown and changing the emergence profile True/False clinical Ideal Preparation for Full Ceramic Restorations Australasian Dentist 61 clinical Article 6 Article AwAiting cPD Point APProvAl from the DentAl boArD. Please refer to our website for updates: www.australasiandentist.com.au fully milled Zirconia crowns (FMZ) by Dr David Penn This new generation of monolithic all zirconia crowns promise so much but impeccable case selection is paramount due to the danger of damaging the opposing dentition. T Dr David Penn he importance of balancing the requirements for strength, aesthetics and avoidance of further tooth wear can be extremely challenging in posterior full coverage restorations. Fundamentally, the rationale driving this choice is based on: 1. The demands on the strength of the restoration/tooth unit 2. Amount of sound tooth structure available 3. Occlusal clearance 4. Aesthetic assessment of the need for translucency versus opacity and 5. Parafunctional activity A further consideration is the abrasiveness of the particular material against natural tooth structure. Ideally, this should match that of natural tooth enamel. It is this interplay between wear, strength and clinical requirements and light transmission, which must be considered when choosing the type of material to be used (Fons-Font et al 2006). Where strength is the prime concern, (virtually in almost every posterior case), as the occlusal loading is high, then clearly a highstrength material is required and the accompanying higher opacity means that aesthetics may have to compromised. As far as abrasiveness is concerned, low-fusing ceramic (e.max, Procera) has been shown to cause less wear of opposing teeth than conventional porcelain (Christenson 2000). It is also well documented that rough, abraded porcelain is extremely damaging to opposing unrestored teeth. One recent study compared various ceramic materials with gold (Elmaria 2006). While gold, unsurprisingly, proved to be the least abrasive, polished lowfusing porcelains also resulted in minimal tooth wear. what about the concept of using zirconia only to make full coverage crowns? Unquestionably, they are very strong compared to more traditional ceramics and in theory at least, its opacity might be useful when trying to mask heavy discolouration. Additionally, these restorations can be fabricated in thin cross-sections, meaning tooth reduction is minimised and conservative “full gold crown” type reparations can be utilised. Patients also prefer a tooth 54 Australasian Dentist clinical coloured restoration where possible and these crowns are generally more aesthetic than full cast metal or metal occlusal surfaces on PFM crowns. Unfortunately, as a stand- alone material for full crowns, it has some significant drawbacks which the manufacturers sometimes gloss over and as there is a paucity of long term in-vivo studies, a cautious approach utilising ideal case selection should be adopted until a body of evidence based research data is available. what is fmZ? FMZ is a new generation fully milled monolithic solid zirconia crown or bridge restoration with no veneering ceramic. The principal qualities of FMZ are: a. Strength and accuracy; designed and milled using CAD/CAM technology, FMZ crowns and bridges are sintered for 6.5 hours at 1,530 degrees Celsius. The final FMZ solid zirconia crown or bridge emerges nearly “bulletproof” with reported compressive strengths of over 1200 mpa. b. No danger of delamination of traditional porcelain veneer layer as with some porcelain fused to zirconia crowns c. Acceptable aesthetics when inserted in lieu of metal occlusal PFM and full-cast metal restorations in the posterior segment d. Virtually chip-proof, it is an ideal restoration for bruxers and grinders, if opposed to metal or other all zirconia restorations e. Conservative preparations similar to FGC are acceptable FMZ crowns and bridges are made from the highest quality zirconia that is uniquely colloidal processed without mechanical pressing or contaminate organic binders for enhanced aesthetics. Other dental zirconia mate- rials on the market today use organic binders to hold the powders together during high pressure pressing to form the milling blanks which diminishes aesthetic properties. laboratory and intra-orally) which is reported to be able to minimise this wear. Other commercially available all zirconia crowns appear to be glazecovered zirconia only which may exacerbate occlusal wear significantly. wear Studies on full-contour Zirconia fmZ indications Recent research from the University of Zurich demonstrates that zirconia which is only glazed and improperly polished can be particularly destructive to opposing tooth structure. Not all zirconia crowns are identical and a number of manufacturers are now using abrasive milled zirconia blocks which are difficult to polish properly and where the glaze is easily removed. FMZir (Southern Cross) has a specific polishing protocol (both FMZ Zirconia crowns or bridges are indicated for bruxers and grinders when PFM metal occlusal or full-cast restorations are not desired and where the antagonist is metallic, zirconia and no dentine is exposed. FMZ is ideally suited for posterior molar crowns when the patient desires a tooth coloured restoration but lacks the preparation space for, or has broken a PFM crown in the past due to bruxing. FMZ can also be utilised for inlays and onlays. Australasian Dentist 55 clinical fmZ contraindications 1. The first problem is that, whilst being very strong, it is also extremely opaque and is therefore only suitable in limited scenarios (posteriors) 2. The second problem is that the fitting surface of a zirconium restoration cannot be etched in the way that materials like e.max or Procera can be and so cannot rely on micro-mechanical 3. Short clinical crowns thus need mechanical retention and further tooth reduction 4. Adjustment of zirconia is difficult and needs specific armamentarium. Extreme heat can be generated and irreversible pulpal damage can occur if not performed correctly. 5. Incorrect and insufficient polishing creates an even more abrasive finish which can wreak havoc with the opposing dentition. If dentine is exposed on the antagonist after adjustment, this wear is exacerbated even further. 6. Removal, especially of inlays, is extremely difficult and can lead to large amounts of tooth destruction 7. Cases where the dentine is exposed on the antagonist pre-operatively should be precluded from FMZ and full gold or PFM options are preferred. Preparation requirements u A full shoulder preparation is not required, chamfer and feather edges are acceptable. u A conservative preparation similar to that for full-cast gold, so any preparation with at least 0.7 mm of occlusal space (1mm is ideal) will work. instructions for Adjustment and Polishing u Adjust FMZ crowns and bridges using water and air spray to keep the restoration cool and to avoid micro-fractures with a fine grit diamond. If using air only, use the lightest touch possible when making adjustments. A football shaped bur is the most effective for occlusal and lingual surfaces; a tapered bur is the ideal choice for buccal and lingual surfaces. u Polishing FMZ restorations is a critical element of this procedure and if not performed properly, can wreak havoc on opposing dentitions. cementation recommendations u Resin reinforced glass ionomer cement (RelyX Luting Cement, 3M ESPE; GC Fuji Plus, GC) u Resin cements for short or overtapered preparations (RelyX Unicem, 3M ESPE; Panavia F2.0, Kuraray) Summary All zirconia crowns have characteristics which are very appealing in many respects. Low biological cost, almost indestructible by nature and tooth coloured characteristics are almost idyllic but these are offset by the need for meticulous case selection. Excessive wear on the antagonist caused by the intrinsic physical abrasiveness of zirconia is problematic and despite the claims of the manufacturers, needs continual vigilance. Long term studies need to be completed before this restoration should be considered for widespread use in the posterior segment. u Dr David Penn is in private practice in Sydney, Australia and is managing director of Southern Cross Dental Laboratories (Australia). Questions for CPD Points True or False 5. FMZ can be bonded to tooth structure effectively? 1. FMZ is an ideal replacement for PFM in the posterior segment in most cases? 6. Bruxers who have metallic or all zirconia antagonists are ideal candidates for this material? 2. All Zirconia blocks are identical in physical and chemical characteristics? 7. Preparations need only be the same as for FG crowns? 3. Excessive wear to the antagonist is the major drawback to this material? 4. Glazing over zirconia will protect the antagonist? 56 Australasian Dentist 8. Removal or adjustment of zirconia can be dangerous to the pulp due to excessive heat generation? 9. Knife edge margins are acceptable? 10. Long term studies need to be completed before utilising? Article 7 clinical Article AwAiting cPD Point APProvAl from the DentAl boArD. Please refer to our website for updates: www.australasiandentist.com.au Aesthetic Failure of Anterior Crowns by Dr David Penn and Dr brenda baker t Dr David Penn he past four decades have witnessed numerous improvements in metal-ceramic and all-ceramic crowns. the initial excitement of the metal-ceramic crown was that it theoretically combined the aesthetics of the porcelain jacket crown with the potential for clinical longevity. shoulder-bevel margins with metal collars were to provide optimal fit and to obtain aesthetics, the metal margins were intended to be hidden within the confines of the gingival sulcus. this concept proved to be rather unpredictable and lead to the development of numerous techniques for fabrication of all-porcelain margins with metalceramic crowns (1). the evolution of such simplified techniques, along with the introduction of several innovative all-ceramic crown modalities has eliminated the need to hide Dr Brenda Baker In an attempt to mask the discoloured dentine, this preparation has a buccal margin that impinges deeply into the sulcus and is likely to be periodontally compromised. 48 AustrAlAsiAn Dentist metal margins deep in the gingival sulcus. However, it is clear that it is impossible to match precisely the shade of the restoration with the colour of the gingival portion of the tooth with these restorations and in most clinical situations it is still desirable to hide the restorative margins underneath the healthy gingival tissues. the exception to this statement is bonded porcelain veneers, where tooth reduction is minimal and the restoration is bonded to sound enamel. in these situations, the contact lens effect allows margins to be placed in a supra-gingival location. However, the disappointment with the metalceramic restorations was the genesis for the development of numerous all-ceramic alternatives to the metal-ceramic restoration (2). Many different techniques for fabricating all-porcelain labial margins are available to improve the inherent aesthetic performance of metal-ceramic restorations. When there is sufficient remaining enamel, etched porcelain laminate veneers may be considered to restore the teeth to optimum aesthetics and function. Failure to obtain optimum results probably has less to do with the restorative medium chosen than it does with failure to adequately prepare the soft and hard tissues to receive the restorations. in order to achieve aesthetic and functional success with any and all of the available modalities, it is imperative that the clinician first bring the gingival tissues to optimal health prior to definitive tooth preparation and maintain this stage of health through the provisional stage. the clinician must understand the nature of the restorative material to be used and prepare the teeth adequately in the correct planes to provide sufficient room for the chosen materials. the dentist must accurately communicate the aesthetic treatment plan to a quality laboratory technician. in spite of these technological improvements, the majority of aesthetic failures with such restorations are biologic. the two primary types of aesthetic failure have been recession of the gingival tissues resulting in exposure of the restorative margins and the presence of chronic marginal gingival inflammation. there are essentials to the soft tissue management inherent in intracrevicular restorative dentistry related to anterior teeth. the clinician faces two basic problems with the soft tissue management. 1. in situations in which the restorative margins are to be placed in the gingival sulcus and are intended clinical to be hidden by healthy gingival tissues the goal is to maintain tissue health and at the same time prevent recession and subsequent exposure of the restorative margin. 2. the restoration has to be placed deep enough in the sulcus to avoid detection and at the same time keep the margin an appropriate distance from the attachment or crest of the alveolar bone so that the biologic width is not violated (3). Preventing gingivAl receSSion Gingival recession in adults is not just a natural effect of aging but rather is a result of pathology. if excellent gingival health is attained prior to definitive margin placement and proper clinical techniques are utilized, the relationship between the prepared restorative margin and the gingival tissues can be very stable, as long as the patient practices proper oral hygiene. there are a number of ways to prevent gingival recession related to anterior crown fabrication, but most of these are under control of the clinician. if excellent gingival health is attained prior to definitive margin placement and appropriate restorative techniques are utilised during therapy, the relationship between the prepared cervical margin and the gingival tissues can be very stable over the long term. this assumes adequate professional maintenance and personal oral hygiene over the long term (4). there are five major strategies for preventing gingival recession when placing anterior indirect restorations, and all are primarily under the clinician’s control. these strategies are: 1. Attaining optimum soft tissue health prior to impression making; Most often patients requiring extensive restoration of anterior teeth do not present with healthy gingival tissues (5). the clinical diagnosis may range from mild gingivitis to chronic periodontitis and it is critical that an accurate diagnosis be made and that the appropriate therapy be initiated. Attainment of optimum soft tissue health prior to determining the final cervical margin location and making the final impression is absolutely critical. With mild gingivitis, the teeth are often prepared, provisional restorations are fabricated and impressions made at the same appointment. this expedited approach is a prescription for disaster. With placement of the definitive restorations a few weeks later, it is reasonable to assume an improved effort on behalf of the patient to comply with oral hygiene procedures, and often in these situations the inflammation in the gingival tissues will resolve or at least be reduced. in this scenario, the gingival tissues will move in an apical direction, often exposing the restorative margins. this can occur during the provisional phase or shortly after the definitive restorations are placed. in either situation, the clinician is faced with an aesthetic failure. the optimum approach is to wait to determine the final margin location when the gingival tissues have attained a state of optimal health. With most anterior restorations, the approach recommended is to prepare the This preparation demonstrates an ideal finishing line with optimal periodontal health. The likelihood of bleeding is minimal and crevicular fluids are well controlled. This recently cemented bridge is already compromised aesthetically. Improved oral hygiene will most likely expose the finishing line and contrast between the ceramic and root surface. teeth after initial scaling and prophylaxis, leaving the cervical margins in a supra or equi-gingival position. excellent indirect provisional restorations must be fabricated, which restore optimum crown and gingival tissue contours, provide access for proper oral hygiene and serve as predictors for the definitive restorations (6,7,8). Gingival enhancement can be achieved by placing the patient on a weak chlorhexidine rinse for 2 weeks (9). the optimal location for the cervical margin in the gingival crevice is determined, and the margin is dropped to this predetermined position. the provisional restorations are relined to restore marginal integrity, impressions are made and the patient continues rinsing with mouth rinse until the definitive restorations are placed. 2. Minimising iatrogenic soft tissue trauma during margin placement and gingival displacement procedures; in order to avoid iatrogenic recession, it is essential that the rotary instrumentation used to drop the cervical finish line to its final intracrevicular position does not damage the soft tissue. retraction cord soaked in water should be placed into the sulcus for 3-5 minutes prior to margin preparation to prevent iatrogenic damage. On removal of the cord, a defined space permits dropping of the margin These failed ceramic veneers were prepared without a finishing line and hence exhibit an emergence profile that is impossible for the patient to clean. The result is accumulation of plaque, chronic gingivitis and a margin that has moved cervically. with minimal chance for trauma. use of rotary instruments especially designed to minimize trauma is recommended. (tissue Protection end cutting burs) it is also critical not to damage the attachment apparatus during gingival displacement procedures. the philosophy of attaining optimum gingival health prior to definitive margin location, coupled with placement of the gingival margin a short distance into the gingival sulcus, permits relatively atraumatic retraction procedures. A suitable diameter retraction cord is placed in the gingival sulcus for eight to ten minutes (10,11). the cord is moistened with water prior AustrAlAsiAn Dentist 49 clinical to removal from the sulcus. Histological evaluation has demonstrated that removal of a dried cord from the sulcus tears the inner epithelial lining, initiates bleeding and may cause irreversible recession (12). An improved retraction system known as traxodent (Premier usA) is now available and yields outstanding results. it offers a convenient way to stop any crevicular seepage as it is impregnated with Aluminium Chloride and is combined with Defining margins with tissue protected end cutting burs minimises iatrogenic periodontal insults. an absorbent clay base which has an affinity towards oral fluid and blood. ideally, it can replace the need for a second cord in the double cord technique as it lessens patient discomfort, displaces the tissue and eliminates the occurrence of break-through bleeding when removing the second cord. 3. Providing provisional restorations of excellent quality; the importance of fabricating quality provisional restorations cannot be overemphasized. these restorations may be made early in the restorative sequence as part of the healing phase or after the preparations are finalized. in either event, such provisionals must demonstrate physiologic crown contours and excellent marginal integrity and provide adequate aesthetics. 4. Eliminating all excess temporary cement; if all-ceramic restorations are planned, a non-eugenol cement should be used to prevent any inhibition of the polymerization of the resin cement with eugenol contained in the zinc-oxide eugenol cements (13). if a conventional dental luting agent is to be used such as glass ionomer or zincphosphate, a zinc oxide-eugenol temporary cement is preferred. While it is now known that zinc oxide-eugenol cements are not obtundent to pulpal tissues, they do provide an excellent initial seal of the prepared tooth. this tends to eliminate sensitivity during the provisional stage. However, zinc oxide-eugenol is a potent soft tissue irritant, 5. Waiting an appropriate time period to allow the tissues to heal after periodontal surgical therapy. When patients require periodontal surgical procedures such as crown lengthening, sufficient time must be allowed after the surgery to permit stabilization of the gingival crest. it is often stated that a waiting period of six to eight weeks is required to attain adequate stability. However, for many patients, this time frame is far too short. in a majority of patients, a waiting period of five to six months is recommended (14). it appears empirically that patients with thin, scalloped gingival tissues are more prone to recession that those with thick, flat tissues. this prolonged waiting period of 5 or 6 months would seem to be essential with the former type of patient. this will mean that many patients will be wearing provisional restorations for protracted lengths of time. it is recommended that such provisional restorations be removed and recemented approximately every six weeks to prevent leakage and subsequent recurrent caries. in summary, recession in association with the placement of anterior restorations is preventable. Attaining optimum soft tissue health prior to final determination of margin location is essential. Atraumatic tooth preparation and gingival displacement procedures are required, along with the fabrication of excellent provisional restorations. A meticulous technique for provisional cementation is critical, and provision must be made for tissue shrinkage after periodontal surgical procedures. gingivAl inflAmmAtion These margins are exposed but the gingival health of this patient has been exemplary. The crowns are twenty years old and demonstrate physiological aging of the periodontium. The two central incisors are implant retained crowns and the periodontal health has been stable for many years. Placement of the fixture in the optimal labio-lingual position is critical as is the provision for correct emergence profile. 50 AustrAlAsiAn Dentist and care must be taken that all excess temporary luting agent is removed from the sulcus prior to dismissing the patient. Any residual cement left in the sulcus will result in gingival inflammation. this inflammatory reaction is reversible upon removal of the irritant, but often a slight amount of recession will occur subsequent to the healing process. this recession, however slight, is detrimental to the long term goal of hiding the margin beneath healthy tissue. Whilst recession exposing the gingival margins has been a primary cause of aesthetic failure with metal-ceramic and all-ceramic restorations, an equally compelling problem is the chronic marginal inflammation in the gingival tissues associated with restorations with subgingival margins. For many years marginal inflammation was attributed to poor oral hygiene, and the patient was admonished to improve oral physiotherapy, usually to no avail. Highly polished metal margins or glazed porcelain margins are smoother and less conducive to plaque accumulation(15). Certain cervical marginal configurations have been demonstrated to be inherently rough and thus to increase the potential for plaque accumulation and retention. therefore, they may contribute significantly to such marginal inflammation. the use of disappearing shoulder margins should be discouraged for this reason. the primary causative factor with chronic gingival inflammation surrounding anterior restorations is violation of the biological width (16). it is tempting for the clinician, who is aiming to prevent margin clinical exposure in the event of some gingival recession to decide to place crown margins deep into the gingival sulcus. Placing the margin deep into the sulcus creates difficulties with gingival retraction and increase the chance that irreversible damage leading to recession might occur. Clinical studies have demonstrated that the closer the restorative margin is to the attachment, the poorer is the periodontal response (17). the further the margin is from the attachment, the better is the periodontal response. specific recommendations have been made to place the restorative margins 0.5 mm from the healthy free gingival margin, or more precisely, a minimum of 3.0 mm from the alveolar crest (18). it is the opinion of the authors that the aetiology of the gingival inflammation seen in the majority of anterior crown restorations is biologic width violation because margins are routinely placed too deep into the sulcus. Often, this results from the clinician not following the anatomical sculpting of the gingival tissues, and the interproximal margins are placed too close to the attachment. While almost all authorities recommend supragingival crown margin placement wherever possible in order to obtain optimum soft tissue health (19). When crown restorations are needed, cervical margins are usually placed in an intracrevicular location as it is usually impossible to blend in crowns imperceptibly with tooth structure when left supragingivally. it is important to consider the patient’s individual smile line and soft tissue display prior to determining the specific margin location when placing anterior restorations. An important tooth-shape criterion for an esthetic smile is the symmetry of the maxillary anterior teeth (20). One excellent study demonstrated that as many as 25 percent of patients do not display the anterior gingival tissues with a normal or even and exaggerated smile. this finding has significant clinical implications in that if patient consent is obtained, many anterior restorations can be placed with supragingival margins, which results in an improved periodontal response, better evaluation of marginal integrity, and substantially simplified operative procedures. in summary, chronic marginal inflammation associated with anterior restorations can be prevented by placing crowns with smooth precise margins in the proper intracrevicular position. that position is quite a short distance into the sulcus (0.5mm) as measured from the crest of healthy gingival tissues. Margins must be a minimum of 3 mm from the alveolar crest and patients must be instructed in and encouraged to perform optimum oral hygiene procedures. An appropriate recall and maintenance program is vital. 5. 6. 7. 8. 9. 10. 11. Summary and conclusions no matter how natural and lifelike anterior restorations may be, the final aesthetic result is particularly dependent upon the health and level of the surrounding gingival tissues. the key to success is effective soft tissue management, and the goal of this soft tissue management has been to provide healthy gingival tissues covering sound, smooth restorative margins. Meticulous attention to detail will result in clinical success regardless of the type of restoration chosen. u 12. 13. 14. 15. 16. 17. bibliogrAPhY 1. 2. 3. 4. Jones DW, Development of dental ceramics. An historical perspective. Dental Clin north Am 1985:29:621-644 Donovan te. Factors successful for allceramic restorations. J Am Dent Assoc 2008 Vol 139: no suppl 4, 14-18s nevins M, skurow HM. the intracrevicular restorative margin, the biologic width, and the maintenance of the gingival margin. int J Periodontics restorative Dent 1984:4:30-39 Kourkouta s. Hemmings KW, laurell l 18. 19. 20. restoration of periodontally compromised dentitions using cross-arch bridges. Principles of perio-prosthetic patient management. nemetz H. tissue management in fixed prosthodontics. J Prosthet Dent. 1974:31:628-636 Cho GC, Chee WWl. Custom characterization of the provisional restoration. J Prosthet Dent 1993 69:529-532 Derbabian K, Donovan te, Marzola r, Cho GC. Arcidiancono A. the science of communicating the art of esthetic dentistry. ii Diagnostic provisional restorations. J esthet Dent 2000:12:238-247 Donovan te, Cho GC. Diagnostic provisional restoration in restorative dentistry: the blueprint for success. J Can Dent Assoc 1999:65:272-275 Marzola r, Derbabian K, Donovan te, Arcidiancono A. the science of communicating the art of esthetic dentistry i. Patient-dentist-patient communication. J esthet Dent 2000:12:131-138 Donovan te, Gandara BK, nemetz H. review and survery of medicaments used with gingival retraction cords .J Prosthet Dent 1985: 53:525-531 nemetz H, Donovan te, landesman HM. exposing the gingival margin. A systematic approach to the control of hemorrhage .J Prosthet Dent 1984:51:647-651 Anneroth G. nordenram A. reaction of the gingiva to the application of threads in the gingival pocket for taking impressions with elastic materials. Odontol revy 1969:20:301-310 rosenstiel s, Gegauff A. effects of provisional luting cements on provisional resins. J Prosthet Dent 1988:59:29-33 Wise MD. stability of gingival crest after surgery and before anterior crown placement. J Prosthet Dent 1985:53:20-23 Wise MD, Dykema rW. the plaque-retaining capacity of four dental materials .J Prosthet Dent 1975:33:178-190 ingber Js, rose lF, Coslet JG. the biologic width: a concept in periodontics and restorative dentistry. Alpha Omegan 1977:70:62-65 Gargiulo AW, Wentz FM, Orban B. Dimensions and relations of the dentogingival junction in man. J Periodontology 1961:32:261-267 Block Pl. restorative margins and periodontal health: a new look at an old problem. J Prosthet Dent 1987:57:683-689 silness J. Periodontal conditions in patients treated with dental bridges. iii the relationship between the location of the crown margins and the periodontal condition. J Periodontal res 1970:5:225-229 Fradeani M. esthetic rehabilitation in Fixed Prosthodontics. Vol 1 Quintessence CPDQuestionnaire Questionnaire CPD (True or False): 1. Gingival recession in adults is a natural effect of aging. 1. The metal-ceramic crown was an initial clinical disappointment to 6. What tissue type makes patients more susceptible to 2. What are the two essentials in soft tissue management in 7. What gingival condition is associated with restorations with 2. Most often patients with healthy gingival tissues. the profession. Why?requiring extensive restoration of anterior teeth present recession? 3. Patients should be placed on weak chlorhexidine for 2 weeks prior to definitive impressions and continue until the definitive restoration is placed. 4. A intracrevicular single retraction cord placed in the sulcus for 8-10minutes combinedsubgingival with Traxodent can replace the double cord technique. restorative dentistry related to anterior teeth? margins? 5. A non-eugenol temporary cement should be used if all-ceramic restorations are planned. 3. Why is excellent gingival health achievement required prior to 8. Why should margins not be placed deep into the sulcus? 6. If definitive patients margin have periodontal placement?surgery, stabilization of the gingival crest occurs within 6-8weeks. 9. How far into the sulcus should the margin be placed? 7. The primary causative factor with chronic gingival imflammation surrounding anterior restorations is violation of the biologic width. 4. How do you avoid iatrogenic recession during tooth preparation? 10.crest. How do you work out the appropriate recall and maintenance 8. Restorative margins should be a minimum of 3mm from the alveolar 5. What is the function of the provisional restoration? program? 9. As many as 25% of patients do not display the anterior gingival tissues with a normal or even exaggerated smile. 10. Patients object to supragingival margin placement anteriorly. AustrAlAsiAn Dentist 51 Article 8 Category CliniCal ARTICLE AwAITINg CPD POINT APPROvAL FROM THE DENTAL BOARD. Please refer to our website for updates: www.australasiandentist.com.au Modern Day Crown Preparations An evidence based examination By Dr David Penn BDs MBA, Head of Clinical and technical research, sCDl and Dr Brenda Baker BDs(Hons) Msc, Director of Clinical education, sCDl t Dr David Penn his three part series of articles identifies principles that can assist dentists design, assess and modify complete coverage preparations to ensure clinical success for the treatment of various unprepared and previously prepared teeth. the individual step by step approach to tooth form preparation will be subsequently reviewed. Finally, troubleshooting of clinical cases will be analysed and causes of failure reviewed. the authors have conducted an extensive search of the literature to provide a detailed “evidence based approach”. PART 1: the form of prepared teeth and the amount of tooth structure removed are important contributors to the mechanical, biologic and aesthetic success of the overlying crown or fixed partial denture. Clinical established guidelines are presented to optimise success and understand the biomechanical implications of physical preparation. Dr Brenda Baker FEATURES AND IMPORTANCE OF PHYSICAL PREPARATION the following features will be reviewed in the preparation characteristics of crowns: 1. total occlusal convergence 2. Occlusalcervical/incisocervical dimension 3. ratio of occlusocervical/incisocervical dimension of buccolingual dimension 4. Circumferential form of the prepared tooth 5. reduction uniformity 6. Finish line location 7. Finish line form 8. Axial and incisal/occlusal reduction depths 9. line angle form 10. surface texture 1. Total Occlusal Convergence total occlusal convergence (tOC) is the angle formed between two opposing prepared axial surfaces. shillingburg et al recently suggested that the tOC should be between 10 and 22 degrees (1). therefore, during clinical tooth preparation, the use of a mirror has been recommended so that a buccal or lingual view of the prepared teeth is established. Buccal/lingual clinical views are the most effective means of assessing tOC because convergence of mesial and distal surfaces is readily visible (2). the dental literature has also presented data on several factors likely to create greater tOC and perhaps even necessitate the formation of auxiliary characteristics that enhance resistance to dislodgement. a. Posterior teeth were prepared with greater tOC than anterior teeth (3,4). b. Mandibular teeth were prepared with greater convergence than maxillary teeth (5,6). c. Mandibular molars were prepared with the greatest tOC (7). d. Buccolingual surfaces had greater convergence than mesiodistal surfaces (3). However, another study (6) determined that mesiodistal convergence was greater than buccolingual convergence. e. Fixed partial denture (FPD) abutments were prepared with greater tOC than individual crowns (8) . f. Monocular vision (one eye) created greater tOC than binocular vision (both eyes) (8). in the presence of the factors that increase tOC beyond the recommended 11 degree to 20 degree range, it is recommended that auxiliary tooth preparation features such as grooves or boxes, be added to enhance the resistance of restorations to dislodgment. Attributes of Single Tooth Permanent Restorations Size of lesion Longevity rating FPD abutment RPD abutment Aesthetics Retention Restoration Protects tooth Replaces Cusp Full-metal crown Large 1 Yes Yes Poor Good Yes Yes Good Poor All Yes Metal-ceramic crown Large 2 Yes Yes Good Good Yes Yes Good Good All Yes All-ceramic crown (veneered) Large 3 No No Excellent Good Yes Yes Adequate Good All Some Full Monolithic Zirconia Large 1 Yes Yes Fair Good Yes Yes Good Poor All Yes Full Monolithic Lithium Disilicate Large 3 Some No Excellent Good Yes Yes Adequate Good All Some 42 AustrAlAsiAn Dentist Occlusal Incisal Buccal Endodontic restoration restoration restoration restoration CliniCal 2. Occlusocervical/Incisocervical Dimension it is proposed that anterior teeth and premolars have a minimal occlusocervical (OC) dimension of 3mm and that molars have a minimal dimension of 4mm. Critical convergence angles have been mathematically calculated and used to identify angles beyond which a crown would theoretically not possess adequate resistance to dislodgement (9,10). An assess ment of the resistance form of dies from clinically failed restorations supported a relationship between convergence angles and clinical failure (11). the resistance of crowns made for dies the size of prepared incisors and premolars has been tested, and it was concluded that 3mm provides adequate resistance(12), supporting the recommended OC dimension for premolars and anterior teeth. the tipping resistance of molarsized crowns has also been measured (13). three millimetres of OC dimension provided adequate resistance but only at 10 degree tOC. three millimetres was inadequate at 20 degree of tOC, an angle frequently found on molars. teeth lacking these minimal dimen sions should be modified to enhance their resistance form through formation of proximal grooves/boxes. rectangular form and most premolars and anterior teeth have an oval form. these shapes produce circumferential irregularity. the value of these irregularities has been evaluated by comparing the resistance areas of conical and pyramidal tooth preparation. the pyramidal preparation provided increased resistance (15). therefore, it is important to preserve the “corners” of a tooth preparation whenever possible. When prepared teeth have no corners due to their round morphologic form or existing condition, they should be modified by forming axial grooves or boxes that provide resistance to dislodging forces. As molars are frequently prepared with greater convergence angles than other teeth and because they usually have a smaller OC dimension and less favourable OC/Bl dimension ratio, they often benefit from axial grooves or boxes. it is suggested that axial grooves/boxes be routinely used when mandibular molars are prepared for bridgework. Chewing and parafunctional habits place dislodging forces on single crowns and fixed partial dentures that are largely Bl in direction, auxiliary resistance form features should be located in the tooth where they provide optimal resistance to these forces. Proximal grooves provided complete resistance to Bl crown dislodgment, whereas buccal or lingual grooves provide only partial resistance (13). therefore, auxiliary resistance form features such as grooves and boxes should be located on the proximal surfaces of fixed partial denture abutments. 3. Ratio of Occlusocervical/ Incisocervical Dimension to Buccolingual Dimension the ratio of the OC dimension to the buccolingual (Bl) dimension should be 0.4 or higher for all teeth. 96% percent of incisor crowns, 92 % of canine crowns, and 81% of premolar crowns possess adequate resistance despite variations in their preparation form and dimensions, However, only 46% of molars possess appropriate resistance (14). When anterior teeth are prepared for complete coverage crowns, they usually possess a favourable ratio between the incisocervical crown dimension and the mesiodistal/buccolingual dimension. Molars have less favorable ratios between the OC dimension and the Bl dimension than anterior teeth. When mandibular molars are prepared they have a rectangular form with rounded corners that enhance resistance form. 4. Circumferential form of the prepared tooth teeth should be prepared so they possess circumferential irregularity whenever pos sible. When teeth are anatomically reduced, they possess characteristic geometric forms. For instance, when prepared maxillary molars are viewed occlusally, they have a rhomboidal form. Mandibular molars have a AustrAlAsiAn Dentist 43 CliniCal 5. Reduction Uniformity teeth should be uniformly reduced, thereby enhancing the potential for normal crown form and an improved aesthetic result. reduction uniformity is best achieved by placing depth grooves into the surface to be reduced and then reducing the tooth in accordance with the grooves. 6. Finish Line Location Finish lines should be positioned equi or supragingivally(16) whenever the aesthetic and resistance form requirements permit such a location. However, subgingival finish lines often are used for appropriate reasons that include the need to achieve adequate OC dimension for retention and resistance form, to extend beyond caries, fractures, and erosion/abrasion;or to encompass a variety of tooth structure defects. subgingival finish lines are also used to produce a cervical crown ferrule on an endodontically treated teeth and to improve the aesthetic result achieved on discoloured teeth. Periodontal health can be retained when subgingival margins are used if other factors must be present. the restorations must be properly contoured and exhibit good marginal fit (17). When a subgingival finish line is required, multiple studies indicate that extension to the level of the epithelial attachment should be avoided. Pocket deepening does not occur when the margin is at least 0.4mm occlusal to the depth of the gingival crevice,(18) whereas more severe gingivitis occurs when subgingival margins approximate the depth of the crevice (19). When teeth were prepared so provisional crown margins were located farther apically than recommended , about a millimetre of gingival recession was noted within 2 weeks and little over 1mm of recession was recorded within 8 weeks (20) . Histologic evaluation indicated the recession mechanism was activated during the first 7 days (20) when crown margins were extended to the bone crest, 1 mm of crestal bone loss was observed (21). 7. Finish Line Form A. All-metal crowns Chamfer finish lines frequently have been used for allmetal crowns. no scientific studies have stated that chamfers are superior to other finish lines. However, they are used with allmetal crowns because they are easy to form with a tapered, round end diamond instrument and because they are distinct, being readily visible on the prepared tooth, impression and die. Chamfers also possess adequate bulk for restorative rigidity and their depth is sufficient to permit the development of normal axial contours. recommended chamfer depth is determined by the minimal metal thickness for strength and minimal space required to develop a physiologic emergence profile. Authors have recommended chamfer finish line reduction depths of 0.3 to 0.5mm (22,23). it is recommended that chamfer finish lines for all metal crowns possess a minimum depth of approximately 0.3mm(2). B. Metal-ceramic crowns the following types of finish line historically have been used with metal ceramic crowns: chamfer, bevelled chamfer, shoulder and bevelled shoulder. recommended metalceramic finish line depths are based on the minimal material thickness required for strength and aesthetics as well as the minimal space required to develop a physiologic emergence profile. A thickness between 1.0 and 1.5mm for the porcelainveneered marginal area of a metalceramic crown has been suggested (1,22,23,24,25). Multiple studies have indicated that at least 1.0mm of translucent porcelain (not including metal and opaque) is required to reproduce the colour of a shade guide (26) which indicates Table 1 Seven Key Principles of Preparation (derived from Shillingberg) Seven space key principles Function Conservation of tooth tissue To avoid weakening the tooth unnecessarily To avoid compromising the pulp Resistance form To prevent dislodgement of a cemented restoration by apical or obliquely directed forces Retention form To prevent displacement of cemented restoration along any of its paths of insertion, including the long axis of the preparation Structural durability To provide enough space for a crown which is sufficiently thick to prevent fracture, distortion or perforation Marginal integrity To prepare a finish line to accommodate a robust margin with close adaptation to minimise micro-leakage Preservation of the periodontium To shape the preparation such that the crown is not over contoured and its margin is accessible for optimal oral hygiene Aesthetic considerations To create sufficient space for aesthetic veneers where indicated 44 AustrAlAsiAn Dentist that tooth reductions in excess of 1.0mm are needed. C. All-ceramic crowns (veneered and monolithic lithium disilicate) Chamfer finish lines produced lower strength with nonbonded crowns in laboratory tests (27). However, the negative effect was not replicated when the crowns were bonded (internally etched crowns cemented to etched prepared teeth with resin) to the teeth (28). it therefore seems appropriate to recommended shoulder finish lines for allceramic crowns that are not to be bonded to underlying tooth structure, whereas chamfer or shoulder finish lines can be used when the crowns are to be bonded. D. All-ceramic crowns (monolithic zirconia) this new generation restoration can be finished with any of the traditional methods: chamfer, bevelled chamfer, shoul der and bevelled shoulder. recommended finish line depths are based on the minimal material thickness required for strength and aesthetics as well as the minimal space required to develop a physiologic emergence profile. Authors and manufacturers have recommended thicknesses between a minimal 0.4 mm and 1.0mm for the marginal area of this monolithic allzirconia crown. 8. Axial and incisal/occlusal reduction depths the required depth of reduction varies with different types of crowns and various surfaces of a tooth. reduction also is affected by the position and alignment of teeth in the arch, occlusal relationship, aesthetics, periodontal considerations and tooth morphology. Deep occlusal interdigitation of posterior teeth or appreciable vertical overlap of the anterior teeth often necessities greater overall reduction of occluding surfaces. Mal aligned teeth commonly have required greater reduction of protruding surfaces to permit restoration alignment and or satisfactory retention and resistance form. Periodontal health is enhanced through the development of normal cervical crown contours, but overcontoured restorations promote plaque accumulation. Allmetal crowns and monolithic zirconia allceramic crowns should have chamfer depths of at least 0.3mm, axial surface reductions of at least 0.5 to 0.8mm and occlusal reduction depths of 1 to 1.5mm (2) . For metalceramic crowns, depths of 1.0mm or more have been proposed and are aesthetically desirable for the finish line and buccal reductions. Finish line (> 1.0 mm) and buccal reductions depths of 1.5 2.0 mm are recommended for veneered and monolithic zirconia allceramic crowns and monolithic lithium disilicate crowns. An CliniCal incisal/occlusal reduction of 2mm for all ceramic crowns permit the development of appropriate colour, strength, translucency and morphology. A. All-metal crowns and monolithic zirconia crowns For allmetal crowns and monolithic zirconia crowns, finish line depths of 0.3 to 0.5 mm have been recommended (22,24). For allmetal crowns and bridges, there are no data that identify the ideal axial reduction depths. the experience of clinicians and laboratory technicians recommends 0.5 at least to 0.8 mm of reduction to be developed near the occlusal aspect of the buccal and lingual surfaces. this depth of reduction provided adequate space for the development of normal axial contours and material thickness for strength. Proximal reduction should include the formation of a distinct finish line and provide access for impression making. A minimum of 1mm of occlusal reduction provides space for the fabrication of these crowns, but reduction depths of 1.5mm provide the space whereby well defined occlusal grooves and convex ridges can be developed. B. Metal-ceramic crowns Finish lines for metalceramic crowns should be 1.0 to 1.5 mm deep and the buccal surface be reduced between 1.0 and 1.7 mm (1,22,24,25). these recommendations are supported by research that determined 1.0mm or more of translucent porcelain is required to reproduce shade guide specimens (26). When aesthetic materials are to be placed over incisal/occlusal surfaces, reduction depths of 2.0 to 2.5 mm have been recommended for metalceramic restorations to provide space for the development of appropriate colour, anatomic form, and occlusion (1,22,23,24). C. All-ceramic veneered crowns and monolithic lithium disilicate crowns Allceramic finish line depth recommenda tions range from 0.5 to 1.0mm (1,22,23,24,25). From a buccal surface reduction perspec tive, there is little improvement in shade matching when the thickness of veneered allceramic crowns or monolithic lithium dislicate allceramic crowns is increased beyond 1 mm with semitranslucent, all ceramic systems (eg. e.Max or empress esthetic) and high value, low chroma shades (eg. A1)(26). However, thicknesses in excess of 1mm are beneficial when using more opaceous allceramic systems (lava 3M esPe or Calypso sCDl) or when using lower value, more chromatic shades such as C2 and A3 (26). the inherent colour of the abutment tooth can influence the colour of the overlying allceramic crown, requiring greater ceramic thickness when the den tine is discoloured. Table 2 Suggested Preparation Features for Posterior Crowns Crown type Posterior Crowns – Preparation Features Occlusal Reduction* Finish Line Depth and Configuration FCC – 1mm non-functional cusps -1.5mm functional cusp 0.3-0.5 mm Chamfer, knife –edge, Shoulder or shoulder with bevel HSAC – 2mm non-functional cusps - 2.5mm functional cusps 1.0 mm shoulder or heavy chamfer PFM – As for FCC if metal occlusal 2mm non-functional clasps 2.5mm functional cusps 1.2mm labial shoulder + or chamfer 0.5mm lingual chamfer (metal collar) 1.2mm circumferentially of 360 degree ceramic margin * Where tooth is tilted or where vertical dimension it to be increased is to be increased, the amount of occlusal reduction required will vary. + Too deep a reduction for diminutive teeth or for long clinical crowns where a metal collar is preferable FCC = Full Contour Crowns (Metal or Zirconia) HSAC = High strength all-ceramic (veneered) or monolithic lithium disilicate PFM = Porcelain Fused to Metal Table 3 Suggested Preparation Features for Anterior Crowns Crown type Anterior crowns – Preparation features Occlusal reduction * Finish line depth and configuration AC 2mm incisally 1mm lingual aspect 0.8-1.0mm shoulder RBPC 2mm incisally 0.5-1.0mm lingual aspect >0.4mm chamfer PFM 2mm incisally 1.2mm labial shoulder + or heavy chamfer 0.5-1.0mm lingual aspect 0.5mm lingual chamfer (Porcelain guidance requires greater clearance) 1.2 mm circumferentially for 360 degree ceramic margin *Where the vertical dimension is to be increased, the amount of occlusal reduction required will be less or non existent. +Too deep a reduction for diminutive teeth eg. Lower incisors or for long clinical crowns where metal collar is preferable) AC : All-ceramic (veneered or monolithic) RBPC: Resin Bonded Porcelain Crowns PFM : Porcelain fused to metal 9. Line Angle Form 10. Surface texture line angles are formed when prepared tooth surfaces meet each other. sharp line angles create stress concentration(27). line angles should be rounded during tooth preparation to enhance strength and minimise crack propagation, especially in allceramic veneered restorations and monolithic lithium disilicate crowns. the purpose of rounding line angles with all metal and metalceramic crowns is related more to facilitating laboratory procedures and optimizing fit than to enhancing restoration strength. round line angles facilitate the fabrication of gypsum casts from impressions without trapping air bubbles as well as the investment of wax patterns without air inclusions. trapped air bubbles can lead to nodules in castings that impede complete seating of a restoration. Casting nodules also are easier to remove when the line angles are rounded during tooth preparation. tooth preparation should be reasonably smooth to enhance restoration fit. tooth preparation smoothness (28) has been found to improve the marginal fit to restorations in two studies whereas another study found no difference in the marginal seating of complete crowns when the axial surfaces were prepared with coarse diamond instruments (120 um grit size) and when they were prepared with fine diamond (50 um grit size) instruments. 11. SUMMARY the following guidelines are proposed when preparing teeth for compete crowns and fixed partial dentures: 1. the tOC (angle of convergence between opposing prepared axial surfaces) should range between 10 degrees and 20 degrees. However, posterior teeth are frequently prepared with greater convergence angles as are fixed denture partial denture abutments. When the tOC angles exceed the recommended AustrAlAsiAn Dentist 45 CliniCal levels, the tooth preparation should be modified to include auxiliary features such as grooves or boxes. tOC and frequently have limited OC dimension and large Bl dimensions that lead to unfavourable ratios. occlusal reduction depths of 2mm are achievable due to the available thickness of tooth structure. 2. three millimetres should be the mini mal occlusocervical/incisocervical (OC/iC) dimension of incisors and pre molars when they are prepared within the recommended tOC range of 10 degree to 20 degree. the minimal OC dimension of molars should be 4 mm when prepared with 10 degree to 20 de gree tOC. When the OC dimension is less than the recommended dimension, the tooth preparation should be modi fied to include auxiliary features such as grooves or boxes. 6. For the purpose of optimizing periodontal health, finish lines should be located equi or supragingivally when the condition of the tooth and aesthetic requirements permits such a location. When subgingival finish lines are required, they should not be extended to the epithelial attachment. 10. rounded line angles on tooth prepara tions for allceramic crowns decrease the stress placed on the crowns and thereby increase crown longevity. With crowns that contain metal (allmetal and metalceramic crowns), line an gles are rounded to facilitate pouring impression and investing wax patterns without trapping air bubbles and to fa cilitate the removal of casting nodules. 3. the ratio of the OC/iC dimension to the Bl dimension should be 0.4 or higher for all teeth. When this ratio is not present, as on large diameter molars, the tooth preparation should be modified to include auxiliary features such as grooves or boxes. 4. teeth should be prepared in a manner that preserves the buccoproximal and linguoproximal corners whenever pos sible because circumferential irregu larities enhance resistance form. When prepared teeth lack “corners” and are round after tooth preparation, they should be modified to include auxiliary features such as grooves or boxes. 5. When auxiliary features are placed into teeth, the preferred locations are the proximal surfaces. the buccal/lingual surfaces are secondary locations to be used when the addition of proximal features leaves the tooth in a state of questionable resistance form. Proximal grooves/boxes should routinely be used when mandibular molars are prepared for bridges because mandibular molars often are prepared with the greatest 7. For allmetal or fully monolithic zir conia allceramic crowns, a minimum 0.3 mm deep chamfer finish lines should be used. the axial and occlusal reduction depths for allmetal crowns should be at least 0.5 mm and 1.0mm, respectively. 8. For metalceramic crowns, finish line selection should be based on formation ease, personal preference, aesthetic requirements and the type of crown being fabricated rather than on expectations of enhanced marginal fit with one type of finish line compared with the others. Many teeth, because of available tooth structure thickness external to the pulp, cannot be reduced buccally to depths that exceed 1mm. 11. tooth preparation smoothness seems to enhance restoration fit, but its effect on retention appears to be related to the type of cement used. surface roughness generally increased retention with zinc phosphate cement, but no definitive relationship has been established when crowns are cemented with adhesive cements (e.g. polycarboxylate, glass ionomer, resin). u For a full list of references, please email [email protected] 9. shoulder finish lines are recommended for allceramic crowns when they are not bonded to the underlying tooth. However, shoulder and chamfer finish lines can be used with all ceramic crowns that are bonded to the prepared tooth using a resin cement and acid etching. Finish line and buccal reduction depths > 1mm are not required when using a semi translucent type of allceramic crown but are beneficial when more opaceous porcelain systems are used or when the tooth structure is discoloured. incisal/ CPDQuestionnaire Questions (True or False): CPD 1. What is the ideal total occlusal convergence(TOC) angle and 7. Circumferential irregularity with tooth preparation enhances Total should with be between 10 and 22 degrees. what important anatomical features? whichocclusal teeth areconvergence frequently prepared greater convergence angles? If this feature has been lost, how is it possible to compensate 2. Buccal lingual clinical views are not the most effective means of assessing total occlusal convergence. for it in the preparation? How isabutments the TOC best assessed clinically? 3.2. Bridge are prepared with greater total occlusal convergence than individual crowns. 8. Where should auxilary resistance form features such as If TOC isteeth exceeded, what is thehave best a way to modify the 4.3. Anterior and premolars minimal occlusocervical dimension of 3mm and be molars a minimal dimension of 4mm. grooves or boxes placed? preparation? 5. Circumferential irregularity is not a beneficial preparation feature.9. What is the recommended finish line and depth for all-metal 4. What are the minimal occlusocervical dimensions for anterior crowns and monolithic disilicate 6. Auxiliary resistance form features such as grooves and boxes should crowns/all-ceramic be placed on buccal and (veneered lingual surfaces of bridge abutments. teeth and premolars and molars? and monolithic zirconia)? 1. 7. Posterior full contour crown either metal or zirconia should have a finish line depth of .3-.5mm 5. What is the ideal ratio of the occlusocervical/incisocervical 10. What finish lines are recommended for all-ceramic crowns 8. The finish line depth of high strength all-ceramic(veneered) or monolithic is .5-1mm. dimension to buccolingual dimension? whenlithium they aredisilicate not bonded to the underlying tooth? What finish lines are recommended for all-ceramic crowns 9.6. The inherent colour ofdo theprepared abutment tooth does not influence the colour of the overlying all-ceramic crown. What geometric forms teeth exhibit? when they are bonded to the prepared tooth using a resin cement and acid etching? 10. Anterior all-ceramic (veneered or monolithic) should have .8-1mm shoulder. 46 AustrAlAsiAn Dentist PERSONAL DETAILS DENTIST NAME: __________________________________ TRADING NAME: _____________________________________ SURGERY ADDRESS: _____________________________________________________________________________________ _____________________________________________________________________________POSTCODE _________________ SURGERY Phone: (_____)___________________ Fax: (_____)___________________Mobile: ___________________________ SURGERY Email: ___________________________________________ A.B.N. ________________________________________ ANSWERS FOR CPD ARTICLES 5- 8 (True or False) Article 8 Article 7 Article 6 Article 5 1 2 1 2 1 2 1 2 3 4 3 4 3 4 3 4 5 5 5 5 6 6 6 6 7 8 7 8 9 7 8 9 7 8 9 10 10 10 RETURN TO sOUTHERN CROSS DENTAL LABORATORIES DR BRENDA BAKER PO Box 607 Double Bay NSW 1360 or FAX: (02) 9362 -1199 EMAIL: [email protected] COURIER ADDRESS: 19 Gum Tree Lane, Double Bay NSW 2028 PO BOX ADDRESS: PO Box 607 Double Bay NSW 1360 PHONE: (02) 9362 - 1177 (6 lines) FAX: (02) 9362 -1199 EMAIL: [email protected] For the latest technical and clinical updates please visit us at www.scdlab.com
© Copyright 2026 ExpyDoc